9-1 copyright © 2008 thomson south-western, a part of the thomson corporation. thomson, the star...
TRANSCRIPT
9-1COPYRIGHT © 2008 Thomson South-Western, a part of The Thomson Corporation. Thomson, the Star logo, and South-Western are trademarks used herein under license.
9-2
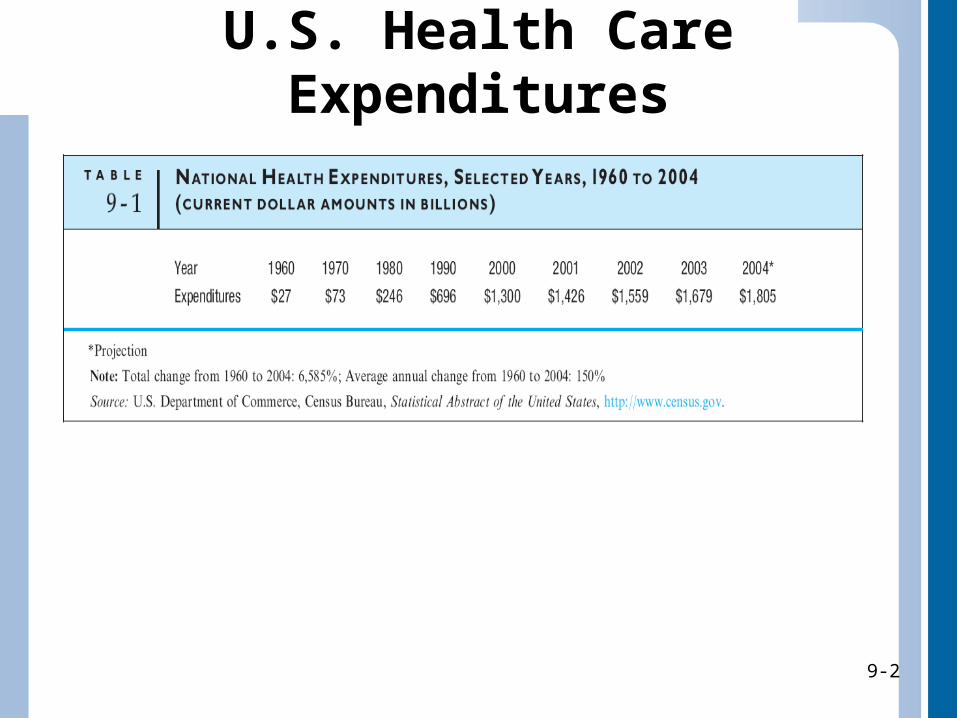
U.S. Health Care Expenditures
9-2
9-3
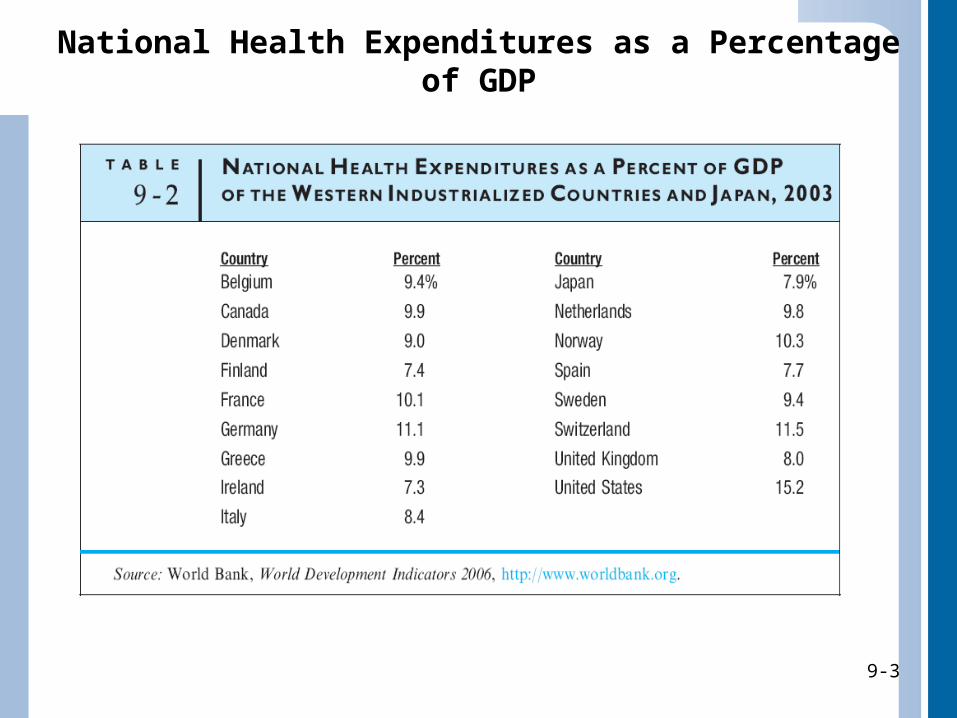
National Health Expenditures as a Percentage of GDP
9-3
9-4
Social Significance of Increased Expenditures
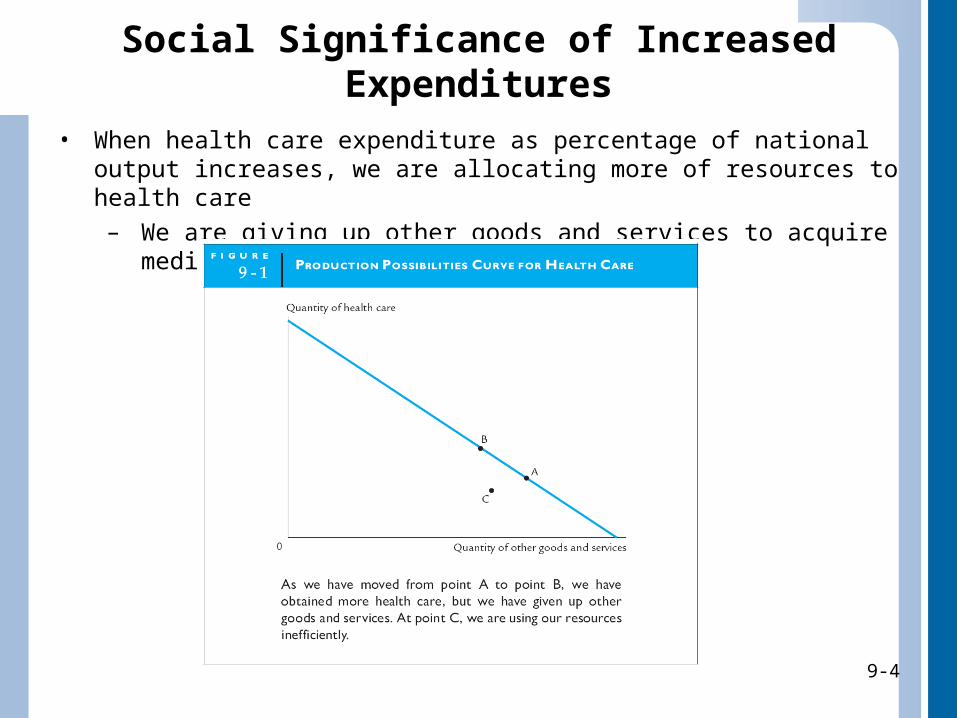
• When health care expenditure as percentage of national output increases, we are allocating more of resources to health care
– We are giving up other goods and services to acquire medical care
9-4
9-5
Health Care Indicators
• Two most commonly used health care indicators are life expectancy at birth and infant mortality rates
– Life expectancy• Age to which a baby born in a particular year can
be expected to live on average
– Infant mortality rate• Number of infants who die before their first
birthday per every 1,000 live births
9-5
9-6
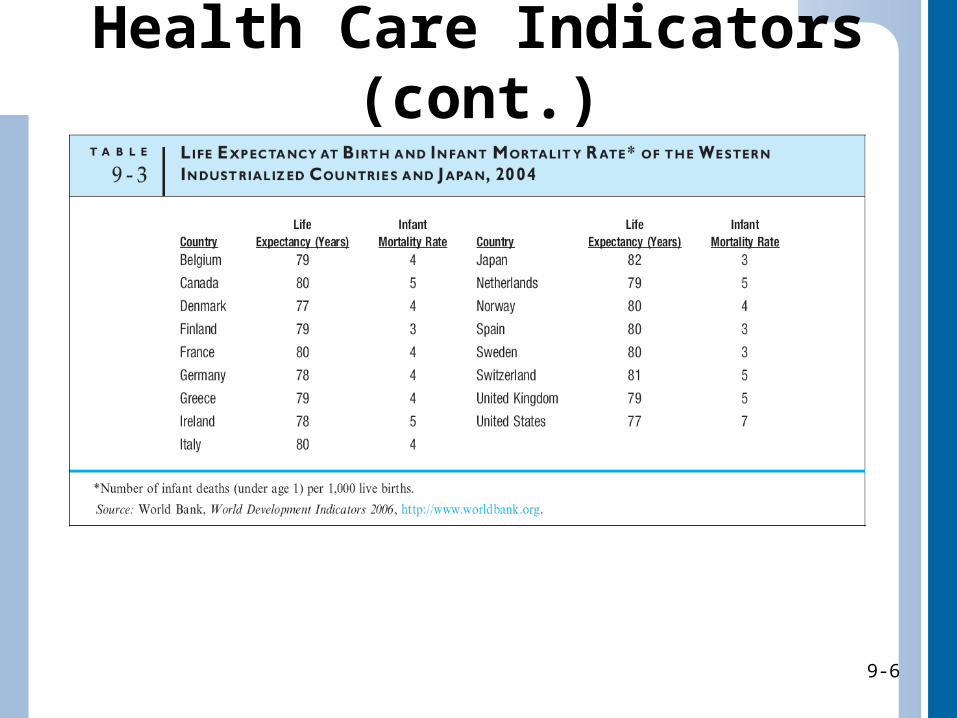
Health Care Indicators (cont.)
9-6
9-7
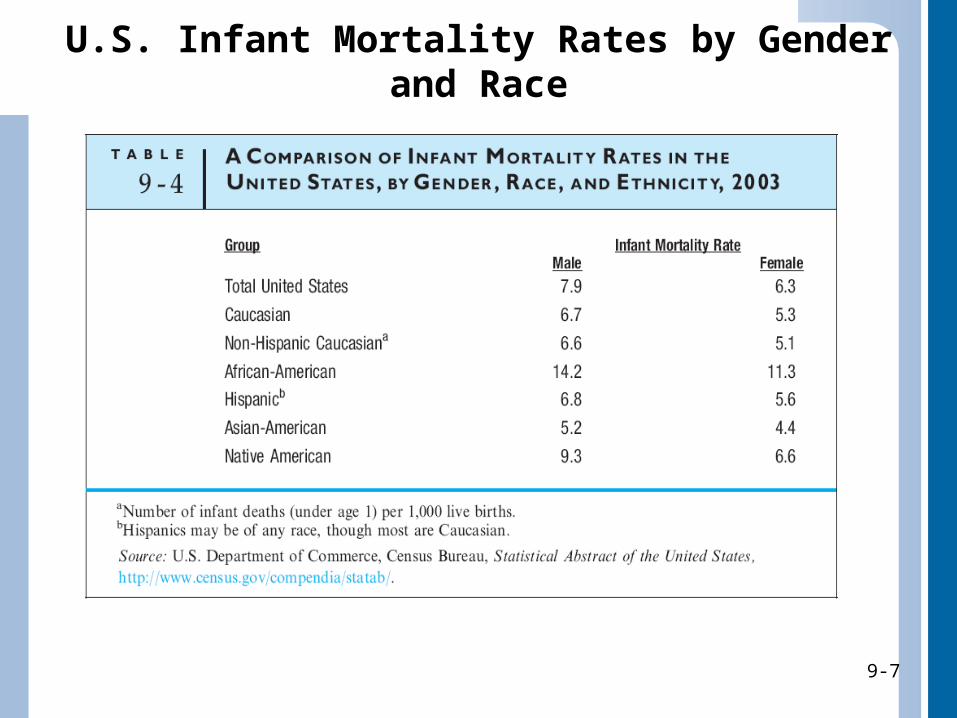
U.S. Infant Mortality Rates by Gender and Race
9-7
9-8
Escalating Health Care Costs
• Reasons why we as nation spend so much on health care are twofold:
1. Consume a growing amount of health care
2. Price of health care is rising
9-8
9-9
Physician Sovereignty• Medical doctor’s control over demand for
medical procedures– We do not shop around for most appropriate medical
care, which contributes to rising health care costs
• Under traditional fee-for-service insurance, more services recommended mean more income the doctor or medical clinic receives– May lead to unneeded services with benefits not
worth costs
• BOTTOM LINE: Physician sovereignty leads to higher demand for medical care, waste, and higher medical costs
9-9
9-10
Third-Party Payment
• Health care payment made by someone other than patient or patient’s family– When third party pays for medical care, we
are more willing and able to ask for additional medical services
• BOTTOM LINE: Third-party payment increases demand for medical care and therefore its price
9-10
9-11
Rapid Technological Change• When hospitals invest in highly specialized
equipment, hospital costs, which have been most rapidly escalating element of health care costs in past 30 years, must then increase
• Many experts believe that expensive and rapidly changing technology is the major force driving hospital costs– Medical experts and their patients judge hospitals by
quality of physicians who are on staffs• Reputable medical doctors choose to practice at hospitals
that have all the latest technology available
9-11
9-12
Inadequate Cost Containment
• Responsibility for containing costs of medical treatment is so diffused that keeping costs down is very difficult
• Hospitals and physicians routinely engage in cost shifting– Recovering unpaid costs of some patients by
charging higher prices to other patients
9-12
9-13
Attitudes of Patients• We believe in high-tech medical system
– Any treatment should be available to us, more tests are better than less, aggressive medical treatment can cure virtually anything, do not need to take much responsibility for our own health• This belief leads us to demand excessive care without much
regard for cost
• We are a litigious society– If we suspect a physician of error, we sue for malpractice
• As a result doctors take out malpractice insurance or protect themselves by practicing defensive medicine– Malpractice insurance
» Insurance carried by health care professionals to protect from large malpractice damage awards
– Defensive medicine» Ordering unnecessary tests and services by health care
professionals solely to protect themselves from charges of malpractice
9-13
9-14
Consequences of These Characteristics
• Have caused medical costs to skyrocket over time
• Physician sovereignty, third-party payment, and increase in tests and treatments caused by rapid technological change and defensive medicine all imply increases in demand for health care
• Installation of new technology and continual replacement of “old” technology, as well as expansion of number of hospital beds and doctors, represent increase in supply of health care
• Consumer advocates maintain that much of our health care expenditures are wasted on unnecessary tests and medical procedures
• Paperwork costs are tremendous
9-14
9-15
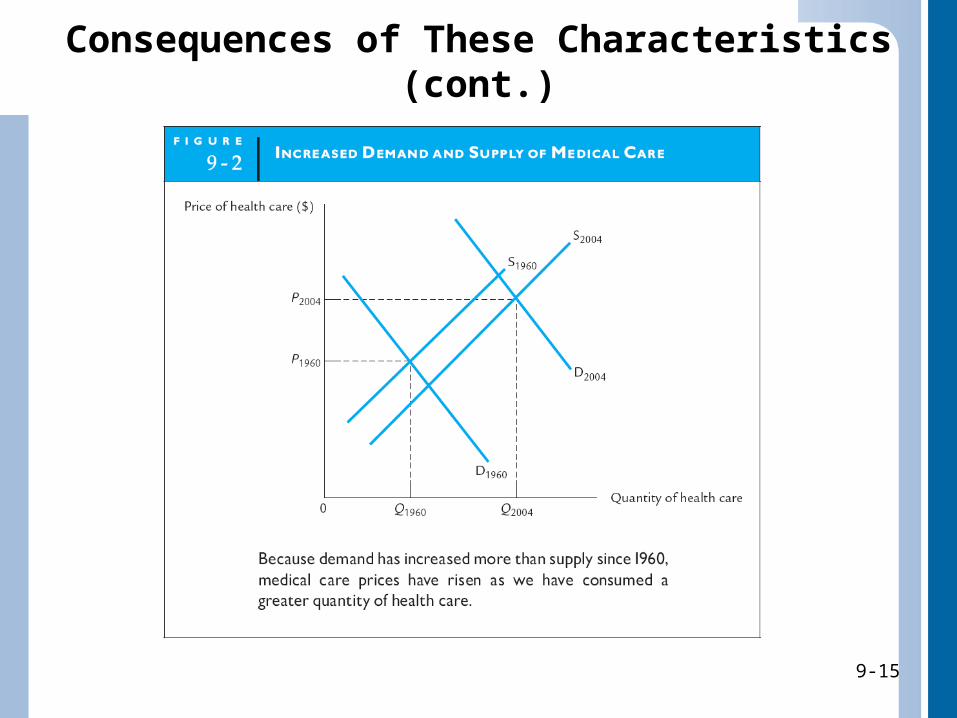
Consequences of These Characteristics (cont.)
9-15
9-16
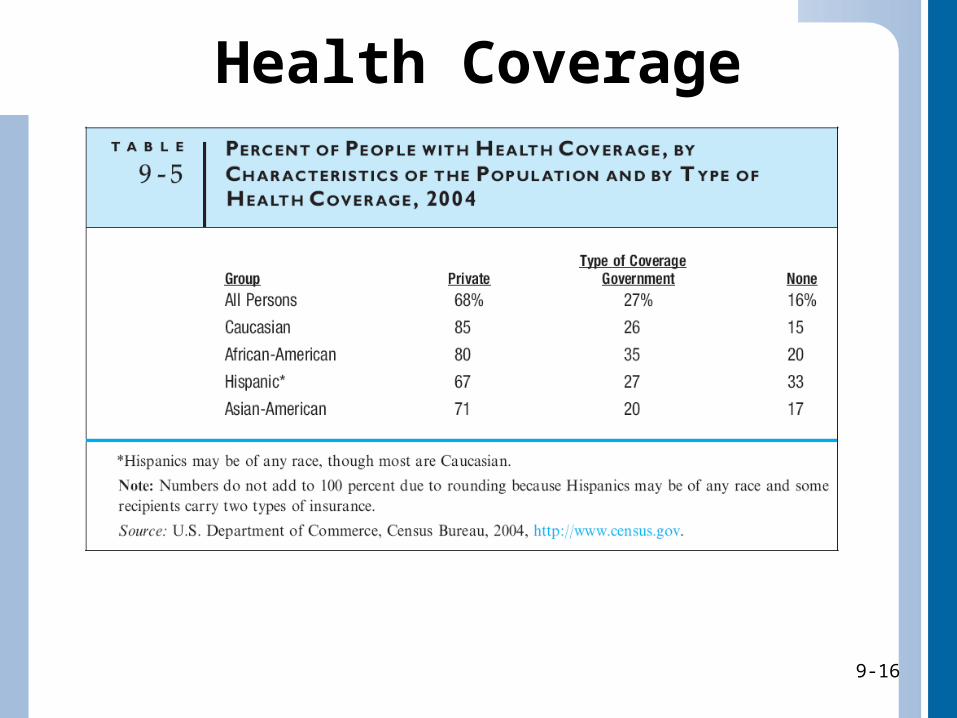
Health Coverage
9-16
9-17
Private Insurance• Patient pays a portion of cost through array of
premiums, deductibles, and coinsurance payments– Premium
• Payment to purchase and keep in force an insurance policy
– Deductible• Payment on annual or per-service basis that must be made
by insured person before insurance company’s payments begin
– Coinsurance payment• Percentage of medical expenses that insured person must
pay over and above deductible
9-17
9-18
Medicaid• Government program providing medical
coverage for eligible low-income people
• Although national in scope, is administered by individual states, and states are free to establish eligibility requirements and benefit levels within certain federal guidelines– Eligibility and coverage vary considerably by state
• Eligibility depends on factors in addition to income, such as age, disability, and assets
– Eligibility does not guarantee access to quality medical care
» Recipients may find it hard to find physicians who will treat Medicaid patients, because government reimburses only a portion of average physician’s fee
9-18
9-19
Medicaid (cont.)• In addition to standard Medicaid program, State
Children’s Health Insurance Program (SCHIP) became available in 1997– Intention is to provide health care to children in
families whose income is too high for children to qualify for Medicaid, but too low for family to afford private insurance
– Jointly financed by federal and state governments and administered by states
• Not all states provide same benefits, but all do include immunizations and care for healthy babies at no cost
9-19

9-20
Medicare• Government program providing medical coverage largely to elderly
people over age 65, as well as certain categories of disabled people• Sponsored by federal government• Medicare hospital insurance (Part A) financed by required payroll
taxes on workers and employers– Includes inpatient care in hospitals, as well as some hospice care and
home health care
• Optional Medicare medical insurance (Part B) for physicians’ services, certain treatments, and other medical services and supplies financed through monthly premiums, co-payments, and deductibles paid by insured person– Because payments never cover full amount of covered services
received by Medicare patients, federal government finances the difference each year
• Optional prescription drug coverage (Part D) began on Jan. 1, 2006– Recipient pays monthly premium for drug coverage, but insurance is
provided entirely by private companies
9-20
9-21
Medicare (cont.)• Because of rising medical costs and increasing
proportion of elderly people in our population, Medicare has become increasingly expensive– Efforts have been made to cut government costs– Premiums paid by recipients have increased,
deductibles have increased, and certain benefits have been cut
• Medicare does not cover all of older people’s medical care– Many older Americans therefore carry expensive
“Medigap” insurance, which covers medical expenses not covered by Medicare
9-21
9-22
Issues with Medicare• Many issues with Medicare are similar to issues
of medical care in general– High and escalating costs, affordability of care, and
access to care (because clinics and hospitals do not have to accept Medicare patients) concern elderly who rely on this program
– Many low-income elderly people refrain from using medical services because they cannot afford deductible or they skip optional portions of Medicare because they cannot afford monthly premiums
– Some important medical services and supplies are not covered at all by Medicare
9-22

9-23
Alternatives for Health Carein the United States
• Given many problems in U.S. health care, there are many proposals for alternative programs– Privatization and increased competition in health care
• Some economists and political scientists want privatization (transfer) of publicly owned hospitals to private sector
– Curtailment or elimination of Medicare and Medicaid• Rising health care costs are partly result of demand not
tempered by usual norms of frugality and concern for price– Because high level of care is reflected in total demand for
medical care, demand would decrease without Medicare and Medicaid, and health care prices would go down
» This withdrawal of medical care from poor and elderly would be deemed unfair by others in society
9-23
9-24
Alternatives for Health Carein the United States (cont.)
– Medical savings accounts• Type of insurance in which purchaser makes
payments into account that can be drawn against in times of illness
– Insured party controls how funds are spent: what tests and procedures are performed, and by whom they are done
– Monies not spent for medical care are returned to insured person, giving him or her stake in minimizing costs of treatment
» Proponents believe accounts would eliminate perverse incentives built into other third-party payment systems
» Critics believe would benefit only relatively healthy people, who would save money on health care
9-24
9-25
Alternatives for Health Carein the United States (cont.)
– Privatization of supply of medical services• Privatized, competitive health care would result in lower costs
– Most hospitals are not run “for-profit”; other goals, such as offering quality overall care, utilizing advanced technology, or specializing in particular services, are paramount
» Critics: Way we finance health care allows hospitals to pursue these goals by shifting uncompensated costs to well-insured patients; privatization of government-owned hospitals and other reforms to increase competition would force them to pay more attention to bottom line, thus eliminating inefficiency
» Supporters: Attack for-profit hospitals for “bottom line” mentality: specialization in high-profit services, neglect of less profitable but important services, cost-cutting measures, and publicized turning away of uninsured and low-income patients
– Advertising within health care industry has been considered unethical
» If prices charged were advertised, competitiveness among suppliers would increase, keeping prices lower
9-25
9-26
Alternatives for Health Carein the United States (cont.)
– Group practices and managed care• May increase efficiency and lower costs:
– Physicians operating in clinic vs. doctor in solo practice– Health maintenance organizations (HMOs)
» Covered care limited to designated providers and use of services coordinated by patient’s primary care physician
– Preferred provider organizations (PPOs)» Group of medical providers contract to provide insured patient’s
medical care at discounted rates
• Managed care rapidly replacing traditional fee-for-service insurance– Major reason is high cost of providing fee-for-service coverage– Growth of managed care and evolving competition among managed
care organizations are credited with slowing growth of U.S. health care expenditures
• Incentive for managed care provider to be cost-efficient– Service costs that “go over contract” would be costly to HMO, while
costs below contracted price would benefit HMO» Services that cut costs in long run, such as health screening,
nutrition and exercise classes are often provided by HMOs– Some worry about quality of care when emphasis is on cost control
9-26
9-27
Alternatives for Health Carein the United States (cont.)
– National health insurance• Government program ensuring universal and
comprehensive coverage of population– Everyone would have health insurance
• United States is in small minority by having no national health insurance program
9-27
9-28
A National Health Plan?• If we wish to extend health coverage to all
people, our desire to cut health care costs will not be possible– On the other hand, not all people need to be
covered by government programs, such as with national health insurance
• National health plan might cover those without access to health care, and high-income and employed individuals might continue to be covered by private insurance
– National plan might pick up catastrophic coverage for individuals with exorbitant medical costs when private benefits run out
9-28
9-29
Benefits and Concerns ofa National Health Plan
• Benefits:– Reduced costs to taxpayers
• Concerns:– Physicians and other health providers might
prefer to treat private patients– Health care providers might shift
uncompensated costs to private insurance companies
– Patients may continue to pay rising out-of-pocket expenses on health care premiums, deductibles, and coinsurance
9-29
9-30
The Economic Left and the Economic Right
• THE ECONOMIC RIGHT (Conservative)– Strongly oppose national
health programs on basis that such programs signify expansion of government’s role
– Favor privatization and increased competition
– Favor trimming Medicare and Medicaid
– Favor development of medical saving accounts
– Urge stronger role for unregulated market
• THE ECONOMIC LEFT (Liberal)– Believe market has done
poor job of allocating medical care
– Argue that special characteristics of health care make it unlikely that market will ever reach fair and equitable solution
– Favor policy ranging from bolstering Medicaid and Medicare to developing national health programs on order of those in other industrialized countries
9-30