6-thalassemia in the american...
TRANSCRIPT

6-Thalassemia in the American Negro
SHLOMOFRIEDMAN, ROBERTW. HAMILTON, and ELuAs SCHWARTZ
From the Children's Hospital of Philadelphia and the Department of Pediatrics,University of Pennsylvania School of Medicine, and the Cardeza Foundationfor Hematologic Research, Jefferson Medical College,Philadelphia, Pennsylvania 19107
A B S T R A C T In Italian patients with high hemoglobinA2 fl-thalassemia trait, the synthesis of P-chains ofadult hemoglobin in the peripheral blood is approxi-mately one-half that of a-chains. In this study the rela-tive rates of f- and a-chain synthesis were determinedin 26 Negro heterozygotes and five homozygotes forfi-thalassemia in six families. The 8/a ratio of globinsynthesis was decreased in only 15 heterozygotes, where-as in the other 11, fl/a globin synthesis was in thenormal range or was slightly increased. These unusualfindings did not appear to be due to the presence ofa-thalassemia or a hyperactive "normal" fl-allele. Thisstudy demonstrates that the f8/a ratio of globin synthesisin the peripheral blood is normal in some patients withP-thalassemia trait. In five Negro homozygotes withrelatively mild clinical disease the f/a ratios were simi-lar to those of Caucasians with Cooley's anemia. Furtherstudies are needed to explore the relationship betweennormal synthesis ratios in many Negro heterozygotesand milder clinical disease in homozygotes in the samefamilies.
INTRODUCTION
fl-Thalassemia trait is a common disorder in the Negro,occurring with an incidence of approximately 0.8% inthe United States (1) and Nigeria (2). Hematologicalfindings including red cell morphology and levels ofhemoglobin A2 (Hb A.) and hemoglobin F (Hb F) aresimilar in Negro and non-Negro patients with P-thalas-semia trait (2-4). Homozygous fi-thalassemia in theNegro has been reported infrequently with approxi-mately 20 cases appearing in the American literature(5). In general these patients have had a milder clinicaldisorder than patients with homozygous fi-thalassemiain other racial groups. The reasons for the generally
Dr. Friedman was the recipient of a U. S. Public HealthService Special Fellowship (HL 54134).
Received for publication 27 November 1972 and in revisedform 22 January 1973.
higher hemoglobin levels and decreased needs for trans-fusion in Negro homozygotes are not known.
We have studied globin synthesis in the heterozy-gotes and homozygotes of six Negro families with f8-thalassemia in order to compare their biochemical find-ings with those seen in other racial groups.
METHODSPatients. Six Negro families that included five patients
with homozygous f8-thalassemia and 26 members with hetero-zygous f8-thalassemia have been studied. The hematologicdata on these patients are summarized in Table I.
The "S" family included two sisters aged 51 and 50 yrwith homozygous fi-thalassemia. The older unmarried sisterhas been anemic all of her life. She has been transfusedregularly with 1 U of packed red blood cells every 2 mosince 26 yr of age. She is short in stature and has markedhepatosplenomegaly and cardiomegaly with compensated con-gestive heart failure. She sustained two fractures of theright humerus and a compression fracture of the body ofa lumbar. vertebra in the past 10 yr, presumably due to aweakening of the bones by excessive hematopoiesis. Theyounger sister was married and had one child. She wasfirst seen in Jefferson Hospital at age 26 for marked cardio-megaly and hepatosplenomegaly with a hemoglobin con-centration of 2.5 g/100 ml. Since then she had been trans-fused on a regular basis with 1i U of blood per mo. In1957 she underwent splenectomy for severe splenic pain and
*hypersplenism. After surgery she did not require bloodtransfusions for 2 yr. In 1970 she began to suffer fromheadaches that were presumably due to pressure from hema-topoiesis in the frontal bones of her skull. The headachesstopped when transfusions were administered more fre-quently. She died recently in cardiac failure due to severehemosiderosis. Ferrokinetic studies in both sisters have beenpreviously reported (6). The pedigree of this family isshown in Fig. 1.
The propositus in the "M" family was a 33-yr old womanwith thalassemia major. At age 20 she was found to havehepatosplenomegaly and a hemoglobin concentration of 4.5g/100 ml. From that time on she received 1 U of blood eachmonth. She had multiple hospitalizations for pericarditis,thrombophlebitis, cholecystitis, and spontaneous abortion.Her operations included removal of an ectopic pregnancy,cholecystectomy, splenectomy, and oophorectomy. In 1967,a chest X-ray examination revealed soft tissue massescompatible with extramedullary hematopoiesis on both sides
The Journal of Clinical Investigation Volume 52 June 1973- 1453-1459 1453

00 )m 4 V m0 if) in4~l N ;,tC) i n - - C4)0 C) 0 Cu) N
~4000~40~0 qO0DO-CC4
4 o Ili _6 r _ o~ e6 a OC U) o
N C, N N(1 N
0000000~~~00' 0000C
o *t- c0 - * 00e r 0go 0 %
00000 06v:
0u J00u)
-~~~~~~+44.t- o4 O - - 0 C-LO M m
a. see(seXeeN
m
_ N0O 0 '_ o 0o0 0%IC4S 0No 0 Go
-ooo-o to _
IDoo o do o- 0o0-
000C~r4o 6 ;( i)COCC)CC4. UC; C-U U)C
OR 0c li aq 0 i I l I" t- In to t- In in mw- if0el; i C- 4 6 l
wo - - o Id! If!eeMiCtnott -
olot0 0 -4 0 tn _ N 0**
CCi VCC)OU° I)0U)0U)C-. C-C-)
00e0U) l Z-O)- - C0C) U0 ag°s t s*ou)
C4C4NN N ~ ~ ~ C4C4 NCN C C-) C- CC) CC NCC) C)C
0 C) Uo) o - UUO u c0r I.0 0 .-00
Nd C )~ -C)C-a 46 d ui i C-i)aC-~- c-) C-C- -
00U)000L c- o - - U U00in *- - o
WCO0 - Co C- ) C-4 " 000 C-e 0 z-.U)
C O 0 0 0 - 0ONco i)_00 00 00 00 n 0
0OR0q1'~C~0 U) liI CO-! c-~o *-'o t-c 0 t-
mLoO In ina tn to t4 4+ _\ i wi+ N o
Ni C! U1 R C!1 C- R C! R Cl R CN _ C- RS C! RSR
o OOUb0Wo00 0 U) r ) es00X+Nr4 r 0 \0a, t- b0N co cor 0 u4IR o t-r r er to W
OO C C)--- C40
0 o00t o. o o o. o\oCeO 0o 0O.O.0o U)~ C O
-4 -o -o0
- -o 0e-
_cu WV
C4 4 bo be be .0beC-__=~~~~~~~~~~~~~~~~~~~~~~ 4 4 4 0 to c OCa S Cs <s 0 CS=OCd Cdd Cd v
~T4 ~ T4 ~ X4 44 L
1454 S. Friedman, R. W. Hamilton, and E. Schwartz
..q
-I*
w
m Cu¢
xerl
C.,
-00 0O
0
0
*0U
9Cd
I._0
-0~
¢cd]0
.0 4)
cdd
¢0
- 0i0 Cd
0
* 440
2 32 4; 5i 64 7El87a
.38 0.63 0.74 1.15 0.76 1.10 1.03
I 2 3 4 5
0.25 0.22 0.95 0.52
m ~ ~~~23 331.09 _ 0.55
f Heterczygous j -Tholassemia
t0>E (High Hb A2)lHeterozygous 6 -Chain Abnormality
@ Normal
D Not Examined
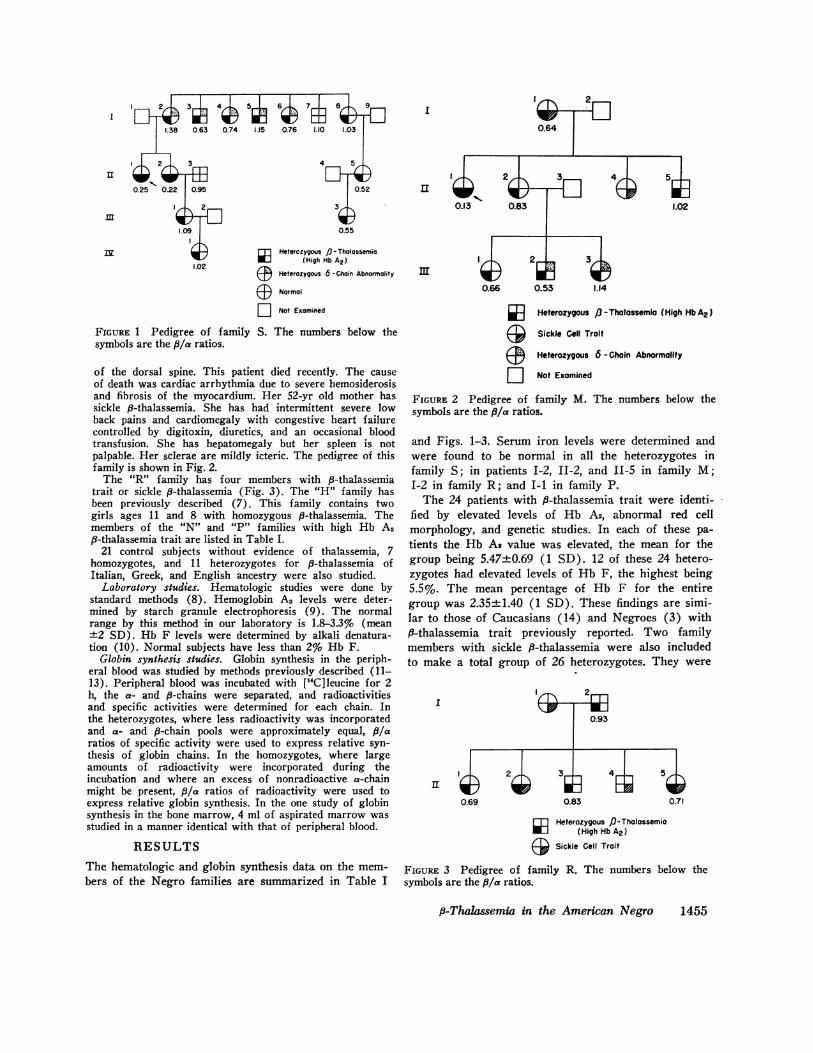
FIGURE 1 Pedigree of family S. The numbers below thesymbols are the f8/a ratios.
of the dorsal spine. This patient died recently. The causeof death was cardiac arrhythmia due to severe hemosiderosisand fibrosis of the myocardium. Her 52-yr old mother hassickle fi-thalassemia. She has had intermittent severe lowback pains and cardiomegaly with congestive heart failurecontrolled by digitoxin, diuretics, and an occasional bloodtransfusion. She has hepatomegaly but her spleen is notpalpable. Her sclerae are mildly icteric. The pedigree of thisfamily is shown in Fig. 2.
The "R" family has four members with f-thalassemiatrait or sickle f8-thalassemia (Fig. 3). The "H" family hasbeen previously described (7). This family contains twogirls ages 11 and 8 with homozygous fi-thalassemia. Themembers of the "N" and "P" families with high Hb A2fi-thalassemia trait are listed in Table I.
21 control subjects without evidence of thalassemia, 7homozygotes, and 11 heterozygotes for f-thalassemia ofItalian, Greek, and English ancestry were also studied.
Laboratory studies. Hematologic studies were done bystandard methods (8). Hemoglobin A2 levels were deter-mined by starch granule electrophoresis (9). The normalrange by this method in our laboratory is 1.8-3.3% (mean±2 SD). Hb F levels were determined by alkali denatura-tion (10). Normal subjects have less than 2% Hb F.
Globin synthesis studies. Globin synthesis in the periph-eral blood was studied by methods previously described (11-13). Peripheral blood was incubated with [14C]leucine for 2h, the a- and u-chains were separated, and radioactivitiesand specific activities were determined for each chain. Inthe heterozygotes, where less radioactivity was incorporatedand a- and f-chain pools were approximately equal, fl/aratios of specific activity were used to express relative syn-thesis of globin chains. In the homozygotes, where largeamounts of radioactivity were incorporated during theincubation and where an excess of nonradioactive a-chainmight be present, f8/a ratios of radioactivity were used toexpress relative globin synthesis. In the one study of globinsynthesis in the bone marrow, 4 ml of aspirated marrow wasstudied in a manner identical with that of peripheral blood.
RESULTSThe hematologic and globin synthesis data on the mem-bers of the Negro families are summarized in Table I
I
II
in
Heterozygous 13 -Tholassemia (High Hb A2)
@ Sickle Cell Trait
@ Heterozygous 6 - Chain Abnormality
D Not Examined
FIGURE 2 Pedigree of family M. The numbers below thesymbols are the f/a ratios.
and Figs. 1-3. Serum iron levels were determined andwere found to be normal in all the heterozygotes infamily S; in patients I-2, II-2, and II-5 in family M;I-2 in family R; and I-1 in family P.
The 24 patients with fi-thalassemia trait were identi-fied by elevated levels of Hb A2, abnormal red cellmorphology, and genetic studies. In each of these pa-tients the Hb A2 value was elevated, the mean for thegroup being 5.47±0.69 (1 SD). 12 of these 24 hetero-zygotes had elevated levels of Hb F, the highest being5.5%. The mean percentage of Hb F for the entiregroup was 2.35±1.40 (1 SD). These findings are simi-lar to those of Caucasians (14) and Negroes (3) withfi-thalassemia trait previously reported. Two familymembers with sickle f8-thalassemia were also includedto make a total group of 26 heterozygotes. They were
I'm,,\ 2m0.93
I
II l;D 2ii& 36 4
El 5;
0.69 0.83 0.71
Heterozygous /J-Thalossemia[l (High Hb A2)
J Sickle Cell Trait
FIGURE 3 Pedigree of family R. The numbers below thesymbols are the ,f/a ratios.
P-Thalassemia in the American Negro 1455

identified by genetic studies, abnormal red cell morphol-ogy, a preponderance of Hb S and a small amount(family R, II-5) or an absence of Hb A (family M,I-1) on electrophoresis. The Negro homozygotes in-cluded three adult patients who needed transfusionsand two children who maintained adequate hemoglobinlevels without therapy. Each of these patients had ele-vated levels of Hb F and abnormalities of red cellmorphology which were similar to those in non-Negropatients.
The mean f8/a ratio in the control group was 0.99±0.05 (1 SD). The Caucasian patients with P-thalas-semia trait and high levels of Hb A2 had a mean fl/aratio of 0.57±0.08 (1 SD). Ratios reported for Cau-casian heterozygotes from other laboratories are similarto those in our group (15-17). The seven Caucasianhomozygotes had a mean fl/a ratio of 0.17, with a rangefrom 0.02 to 0.25. Ratios in homozygotes reported byother laboratories ranged from 0 to 0.24 (15-19).
The values of the f/a ratios in the Caucasian groupwith 8-thalassemia trait did not overlap those of thecontrol group. In contrast, the fl/a ratios of the Negrogroup with heterozygous fl-thalassemia ranged from0.52 to 1.38, overlapping the Caucasian heterozygotesand the control group (Fig. 4). 11 of the 26 Negro pa-tients had f/a ratios within the normal range or above.The mean fl/a ratio of the Negro group was 0.84±0.21(1 SD).
The fl/a ratios in the five patients with homozygousfl-thalassemia ranged from 0.13 to 0.25, values similarto those found in Caucasians. Studies of globin synthesisin the bone marrow of two of these patients (family"H", daughters 1 and 2) have been previously re-
6-THALASSEMIA | -THALASSEMIA CONTROLSMAJOR TRAIT
CAUCASIAN NEGRO CAUCASIAN NEGRO
1.4-
1.2
0Z 1.0 .e.
cit~~~~~~~~~~~~~v0O.8-3
0.60
0.4-
0.2 -4
FIGURE 4 8/a Ratios in the five groups studied. The meanof each group is indicated by a horizontal line.
ported (7) and were also found to be similar to thosein Caucasian patients.
Peripheral blood and bone marrow studies were doneon one Negro heterozygote (family "S", I-8). The fl/aratio in the peripheral blood was 1.03, and that in thebone marrow was 1.13. There was 22 times as muchradioactivity incorporated in the bone marrow sampleas in the same volume of peripheral blood. There wereadequate iron stores in the marrow.
Studies of three Negro patients were repeated on asecond occasion to test the constancy of the unusualfindings in this group. The results using the samemethods have been found to be highly reproducible inour laboratory and by others (17). The paired resultsin patients 1-2 and I-8 from family "S" and the motherfrom family "P" were 1.38 and 1.36, 1.03 and 1.02, and0.69 and 0.68, respectively. The second study in thefirst two patients was done 2 yr after the first study,while the interval for the third patient was 2 mo. Theseresults indicate that the f8/a ratios in these patients,whether high, normal, or low, did not vary with time.Two chromatographic studies are shown in Fig. 5.
Several patients in families S and M were found tohave Hb A2', a 6-chain variant found commonly inNegroes (20) (Figs. 1, 2). The Hb A2 values givenfor these patients (Table I) are the sum of the Hb A2and Hb A2' bands on starch block electrophoresis.
DISCUSSIONfl-Thalassemia is an inherited disorder of hemoglobinsynthesis found in many ethnic groups, including Ital-ians, Greeks, Turks, Arabs, Indians, Southeast Asians,and Chinese. The most common heterozygous form ofthis disorder is associated with hypochromia, microcy-tosis, an elevated red cell count, and a high level ofHb A2. In many of the patients with elevated Hb A2,there is also a mild elevation of Hb F. Although theheterozygotes are usually asymptomatic, they may havemild anemia. The clinical features of fl-thalassemia traitin the Negro do not seem to differ from those seen inother ethnic groups. The mean Hb A2 level in the 24Negro heterozygotes in this study was 5.5%, a valuesimilar to those of Negro heterozygotes (5.1%) previ-ously reported (3). The mean Hb F level (2.3%) andthe range of Hb F are also similar to those previouslyreported (3).
Homozygotes for P-thalassemia in the non-Negrogroups usually have severe clinical disease which startsin the 1st yr of life, requires frequent blood transfusionsand results in death during or before the third decadeof life. In contrast, most Negro homozygotes have arelatively mild disease, frequently live to the fourthdecade and beyond and occasionally give birth withuneventful pregnancies. Although some of the patients
1456 S. Friedman, R. W. Hamilton, and E. Schwartz

24
24
1
a
4
E
"I.
C-
0
0
4
cr
.2
1.0
0.8
0.6
WL 4 E
~~~~~~~~~~~CI ~~~~~~~0
301- Q2CD
0 ,0Ip110ja.0 to 15 20 25 30 35 40 45
PO- 1.2 14
*A°il D. Orw
TUBE NUMBER
FIGURE 5 Chromatograms of globin from patients I-8 (A) and II-5 (B) in family S. The,8/a specific activity ratios in these Negro patients with high Hb A2 are 1.02 (A) and 0.52(B). The first patient was studied on separate occasions 2 yr apart, with similar results eachtime.
do not need regular transfusions, others may developsymptoms of severe anemia in the third or fourth decadenecessitating the initiation of a regular transfusion pro-
gram (21). The three Negro adult patients reportedhere were well until they were approximately 20 yr old,when decreasing hemoglobin levels necessitated trans-fusion therapy on a regular basis. The prognosis ofyoung Negro children with homozygous P-thalassemia istherefore guarded, despite relative well-being earlier inlife. The reason for the generally milder clinical diseasein Negro patients and the deterioration in some of themas they grow older is not known.
In normal persons there is equal synthesis of a- and$-chains in peripheral blood reticulocytes. In Caucasianswith heterozygous P-thalassemia, the synthesis of f-
chain is approximately one-half that of a-chain in theperipheral blood (15-17). The results of peripheralblood studies in the Negro heterozygotes reported herediffer markedly from those in Caucasians. Reports of
unexpected results in Negro heterozygotes have alsorecently appeared in abstracts (22, 23). Only 58% ofthe Negro patients in our studies had deficient f8-chainsynthesis, whereas the remainder were in the normalrange (mean ±2 SD) or above. These two groups ofNegro heterozygotes could not be distinguished by dif-ferences in hemoglobin concentrations, red cell indices,Hb A2 or Hb F levels. Repetition of the globin syn-
thesis studies in three patients with high, normal, or
low f/a ratios, as well as in other patients studied inout laboratory, indicates that the results are reproducibleand are characteristic of globin synthesis in any patient.
An analysis of the pedigrees shows the distribution ofdifferent globin synthesis ratios within individual fami-lies. Both types of patients with fl-thalassemia trait (lowfl/a ratio, normal f8/a ratio) are found in each of three
families (Figs. 1-3). In another family (H) all highHb As heterozygotes had globin synthesis ratios withinthe range of normal controls, although in a fifth family
p-Thalassemia in the American Negro 1457
40- A p '%-0.D.
60t - cpm 0A
, N

(N) both heterozygotes had low P/a ratios (Table I).In family "S", patient 1-8 had a normal 8/a ratio,whereas her daughter (II-5) and granddaughter (III-3) had ratios of approximately 0.5 (Fig. 1). Thesefindings could possibly be due to the presence of botha-thalassemia and 8-thalassemia in patient I-8, with alack of transmission of a-thalassemia to her daughter.In both Italian and Chinese patients, doubly heterozy-gous for a- and 8-thalassemia, the P/a ratios haveranged from 0.95-1.03 (17). Further analysis of family"S" indicates that unusual ratios were most probablynot due to the modifying influence of a-thalassemia. Pa-tient I-2 with 9-thalassemia trait had a high ratio of1.38, whereas her two daughters (II-1, 11-2) with homo-zygous P-thalassemia had 8/a ratios of 0.22 and 0.25, inthe range of those found in Caucasians with Cooley'sanemia (15-19) (Fig. 4). The daughter (III-1) andgranddaughter (IV-1) of one of the homozygous pa-tients (II-2) had balanced globin synthesis. In anItalian patient with homozygous 8-thalassemia andheterozygous a-thalassemia and a relatively mild clinicaldisorder, the 8/a ratio was 0.45, indicating the modify-ing effect of the a-thalassemia gene on the expressionof the two P-thalassemic genes (17). The globin syn-thesis ratios in the two Negro homozygotes in family"S" show no evidence of a modifying effect of an a-thalassemia gene. The daughter (III-1) of one homo-zygote inherited a gene for 8-thalassemia from hermother but did not inherit a-thalassemia from eitherher mother (8/a = 0.22) or father (,8/a = 0.95). Thenormal globin synthesis ratios in patients III-1 andIV-1 thus are not due to the presence of a-thalassemia.Indeed, it would be highly unlikely to find a-thalassemiatrait in 42% of the 8-thalassemia heterozygotes in thisstudy, when the incidence of a-thalassemia in the Negrois approximately 2% (24). No patients with simple a-thalassemia trait were found in any of the Negro fami-lies included in this study. The presence of an inter-acting gene for the silent carrier state of a-thalassemiain some of the patients could not be ruled out by thesestudies.
Itano (25) has postulated the existence of severalnormal globin chain alleles which differ in their syn-thetic capacities. The presence of a hyperactive 8-chainallele in the trans position to the thalassemic gene insome heterozygous patients might explain the occur-rence of balanced globin synthesis ratios in these pa-tients. A single gene of this type does not seem to havebeen present in the two largest families studied (familiesS and M). In both of these families there is an abnormal8-chain in some individuals which serves as a markerfor the 8P-loci. Patients 1-2 and I-5 in family "S" (Fig.1) had the abnormal 8-chain and unusually high 8/aratios for ,-thalassemia, whereas siblings I-3, I-4, and
1-6 had low P/a ratios and also possessed the abnormal8-allele. In family "M" (Fig. 2) one sibling with anabnormal 8-chain (III-2) had a P/a ratio of 0.53, where-as a sister with the same 8-variant (III-3) had a ratioof 1.14. It is thus unlikely that a "super-gene" producedsynthesis in some of the Negro patients, since the P-and 8-loci are closely linked (26), and the factor pro-ducing balanced synthesis is not linked to the 8-locus.
A recent study of a-thalassemia in the Negro con-cludes that there is a much wider range of a/P syn-thesis ratios than in Caucasian patients (27). The valuesin the Negroes overlap the normal range, and theaverage ratio indicates less imbalance of globin synthe-sis than in the Caucasian group. The results of thestudies reported in this paper demonstrate a similarfinding in 8-thalassemia trait in the Negro. The mean
P/a ratio is higher than in Caucasians, and many pa-tients have ratios in the normal range.
Although Caucasian heterozygotes for 8-thalassemiahave a relative decrease in synthesis of P-chains intheir peripheral blood, P- and a-chain synthesis areequal in the bone marrow (28). The presence of bal-anced globin chain synthesis in the bone marrow sug-gests that compensatory P-chain synthesis for the thalas-semic defect is present in the nucleated red cells ofsome patients. The possibility that decreased P-chainsynthesis was present in the bone marrow but not in theperipheral blood of the Negro heterozygotes with un-usually high ratios was tested in one patient (family S,I-8). Unbalanced globin synthesis was not detected ineither bone marrow or peripheral blood of this patient,the P/a ratios being 1.13 and 1.03, respectively. It hasbeen suggested that the difference previously observedin globin synthesis between bone marrow and peripheralblood cells in heterozygotes might be due to the in-creased rate of breakdown in the red cell of messengerRNA for P-chain (28) either from the thalassemic orthe normal P-chain locus. The factors responsible forbalanced globin synthesis in some of the Negro hetero-zygotes may act by protecting the messenger RNAforP-chain from an excessive rate of decay. In heterozy-gotes with decreased mean cell hemoglobin values andeither balanced or unbalanced globin synthesis in theperipheral blood, the total amount of a-chain per cell isdecreased as well as the amount of 8-chain suggestingthat there may be depression of synthesis of a-chain inthe bone marrow in some patients as part of the compen-satory changes occurring in the nucleated erythrocyte.
The difference in severity of clinical disease in theNegro and Caucasian homozygotes is not reflected indifferences of peripheral blood or bone marrow (7) P/aratios. Further studies are needed to clarify the rela-tionship of the biochemical differences in the heterozy-gotes to the clinical differences in the homozygotes.
1458 S. Friedman, R. W. Hamilton, and E. Schwartz

ACKNOWLEDGMENTSWe wish to thank Dr. I. Robert Schwartz for referringfamily P, and Jean Atwater for determinations of Hb Asand Hb F.
This work was supported by U. S. Public Health Servicegrant AM 16691 and a grant from the Cooley's AnemiaFoundation.
REFERENCES1. Goldstein, M., A. Patpongpanij, and V. Minnich. 1964.
The incidence of elevated hemoglobin As levels in theAmerican Negro. Ann. Intern. Med. 60: 95.
2. Esan, G. J. F. 1970. The thalassemia syndromes inNigeria. Br. J. Haematol. 19: 47.
3. Weatherall, D. J. 1964. Biochemical phenotypes of thal-assemia in the American Negro population. Ann. N. Y.Acad. Sci. 119: 450.
4. Huisman, T. H. J., W. A. Schroeder, S. Charache, N.C. Bethlenfalvay, N. Bouver, J. R. Shelton, J. B. Shel-ton, and G. Appell. 1971. Hereditary persistence of fetalhemoglobin. N. Engl. J. Med. 285: 711.
5. Crouch, E. R., Jr., H. M. Maurer, and 0. S. Valdes.1970. Probable homozygous beta thalassemia in a Negrochild. Am. J. Dis. Child. 120: 356.
6. Haurani, F., G. Bain, G. Wang, and L. M. Tocantins.1960. Erythrokinetic studies in thalassemic hemoglobinop-athies before and after splenectomy. Haematol. Lat. 3:1.
7. Friedman, Sh., F. A. Oski, and E. Schwartz. Bonemarrow and peripheral blood globin synthesis in betathalassemia in a black American family. Blood. In press.
8. Cartwright, G. E. 1963. Diagnostic Laboratory Hema-tology. Grune & Stratton, Inc., New York. 3rd edition.
9. Gerald, P. S., and L. K. Diamond. 1958. The diagnosisof thalassemia trait by starch block electrophoresis ofthe hemoglobin. Blood. 13: 61.
10. Singer, K., A. J. Chernoff, and L. Singer. 1951. Studieson abnormal hemoglobins. II. Their identification bymeans of the method of fractional denaturation. Blood.6: 429.
11. Clegg, J. B., M. A. Naughton, and D. J. Weatherall.1965. An improved method for the characterization ofhuman hemoglobin mutants: identification of a2nG~LUhemoglobin N (Baltimore). Nature (Lond.). 207: 945.
12. Kan, Y. W., E. Schwartz, and D. G. Nathan. 1968.Globin chain synthesis in the alpha thalassemia syn-dromes. J. Clin. Invest. 47: 2515.
13. Schwartz, E. 1969. The silent carrier of beta-thalas-semia. N. Engl. J. Med. 281: 1327.
14. Beaven, G. H., M. J. Ellis, and J. C. White. 1961.Studies on human fetal hemoglobin. III. The hereditaryhemoglobinopathies and thalassemia. Br. J. Haematol.7:169.
15. Bank, A., and P. A. Marks. 1966. Excess a chain syn-thesis relative to 8 chain synthesis in thalassemia majorand minor. Nature (Lond.). 212: 1198.
16. Weissman, S. M., I. Jeffries, and M. Karon. 1967. Thesynthesis of alpha, beta, and delta peptide chains byreticulocytes from subjects with thalassemia or hemo-globin Lepore. J. Lab. Clin. Med. 69: 183.
17. Kan, Y. W., and D. G. Nathan. 1970. Mild thalassemia:the result of interactions of alpha and beta thalassemiagenes. J. Clin. Invest. 49: 635.
18. Weatherall, D. J., J. B. Clegg, and M. A. Naughton.1965. Globin synthesis in thalassemia: an in vitro study.Nature (Lond.). 208: 1061.
19. Conconi, S., A. Bargellesi, S. Poutremoli, V. Vigi, S.Volpato, and D. Gaburro. 1968. Absence of ,-globin syn-thesis and excess of a-globin synthesis in homozygous,B-thalassemia subjects from the Ferrara region. Nature(Lond.). 217: 259.
20. Horton, B., R. A. Payne, M. T. Bridges, and T. H. J.Huisman. 1961. Studies on an abnormal minor hemo-globin component (Hb B2). Clin. Chim. Acta. 6: 246.
21. Pearson, H. A., and W. D. Noyes. 1964. Thalassemiaintermedia. Cases in Negro siblings with unusual differ-ences in minor hemoglobin components. Blood. 23: 829.
22. Hamilton, R., and E. Schwartz. 1970. Equal synthesis ofa and fl-chains in a Negro family with 8 thalassemia.Am. J. Hum. Genet. 22: 12a.
23. Braverman, A., P. R. McCurdy, and 0. Manos. 1971.Mild homozygous 8-thalassemia in Negroes. Clin. Res.19: 407.
24. Weatherall, D. J. 1963. Abnormal hemoglobins in theneonatal period and their relationships to thalassemia.Br. J. Haematol. 9: 265.
25. Itano, H. A. 1953. Qualitative and quantitative controlof adult hemoglobin synthesis-a multiple allele hypothe-sis. Am. J. Hum. Genet. 5: 34.
26. Schwartz, E., D. Smith, and D. G. Nathan. 1967. Loci ofhuman hemoglobin genes. Lancet. 2: 1422.
27. Schwartz, E., and J. Atwater. 1972. Alpha thalassemiain the American Negro. J. Clin. Invest. 51: 412.
28. Schwartz, E. 1970. Heterozygous beta thalassemia: bal-anced globin synthesis in bone marrow cells. Science(Wash. D. C.). 167: 1513.
p-Thalssemia in the American Negro 1459