1. introductionshodhganga.inflibnet.ac.in/bitstream/10603/3488/12/12_chapter 1.pdf · 1.1.3....
TRANSCRIPT
1. INTRODUCTION
The idea of developing mucoadhesive polymers for drug delivery
has been introduced into the pharmaceutical product development for
more than 40 years ago and nowadays it has been subjected as a
promising strategy to improve the residence time and the specific
localization of drug delivery systems on various mucus membranes.
The term bioadhesion may be defined as a condition in which two
materials are held together for extended periods of time by interfacial
forces, out of which one material is in biological nature. In the
pharmaceutical literature, when the adhesive attachment is to mucus
or a mucous membrane, the phenomenon is classified as
mucoadhesion1.The mucoadhesive formulations have been
successfully used for the effective delivery of drugs for systemic
action/localized action and also to deliver the difficult molecules
(proteins and oligonucleotides) into the systemic circulation.
1.1. Mucoadhesion
For the last two decades the research on mucoadhesion has
become of interest because of its usefulness in improvising the
localized drug delivery, by retaining a formulation at the site of action
(e.g. within the gastrointestinal tract) or systemic delivery, by retaining
a formulation in intimate contact with the absorption site (e.g. the
nasal cavity). Moreover the mucoadhesive materials could also be
used as therapeutic agents by coating and protecting damaged tissues
(gastric ulcers or lesions of the oral mucosa) or by acting as
lubricating agents2 (in the oral cavity, eye and vagina).
1.1.1. Structure of mucus membrane
Mucus membranes (mucosa) are the moist surfaces lining the
walls of various body cavities such as the gastrointestinal and
respiratory tracts. The mucus consists of a connective tissue layer (the
lamina propria) above which is an epithelial layer and the mucus layer
makes the surface moist. The epithelia of mucosa may be either single
layered (e.g. the stomach, small and large intestine and bronchi) or
multilayered/stratified (e.g. in the esophagus, vagina and cornea). The
former contain goblet cells which secrete mucus directly onto the
epithelial surfaces, the latter contain, or are adjacent to tissues
containing, specialized glands such as salivary glands that secrete
mucus on to the epithelial surface. Mucus exists either as a gel layer
adherent to the mucosal surface or as a luminal soluble or suspended
form. The composition of mucus gels consists of mucin glycoproteins,
lipids, inorganic salts and water. The water portion accounts for more
than 95% of its weight and makes it a highly hydrated system3. The
mucin glycoproteins are the most important structure-forming
component of the mucus gel and are responsible for its characteristic
gel-like, cohesive and adhesive properties. The thickness of this
mucus layer varies on different mucosal surfaces, from 50 to 450 µm
in the stomach4-5 to less than 1 µm in the oral cavity6. The major
functions of mucus are that of protection and lubrication (they could
be said to act as anti-adherents).
1.1.2. Mechanisms of mucoadhesion
For the occurrence of mucoadhesion, the molecules must
involve in bond formation across the interface. The mechanism of
bond formation is varied and can be divided into following ways. (1)
Ionic bonds—In this the two oppositely charged ions comes together
through electrostatic interactions and forms a strong bond (e.g. in a
salt crystal). (2) Covalent bonds—this bond forms by sharing the
electrons, in pairs, between the bonded atoms in order to fill the
orbitals in both.
(3) Hydrogen bonds—here a hydrogen atom, when covalently bonded
to electronegative atoms such as oxygen, fluorine or nitrogen, carries
a slight positively charge and is therefore is attracted to other
electronegative atoms. The hydrogen bond considered to be weaker
than ionic or covalent bonds. (4) van der Waals bonds—this bond is
because of interaction that arise from dipole–dipole and dipole-
induced dipole attractions in polar molecules, and dispersion forces
with non-polar substances. 5) Hydrophobic bonds—this is a indirect
way of bond formation occurs when non-polar groups are present in
an aqueous solution by hydrophobic effect.
1.1.3. Theories of adhesion
There are six general theories of adhesion, which have been
adapted for the investigation of mucoadhesion7-8.
1) The electronic theory indicates the transfer of electrons between
the materials and adhering surface because of differences in the
electronic structure. This is proposed to result in the formation of an
electrical double layer at the interface, with subsequent adhesion due
to attractive forces.
2) The wetting theory is defined by surface and interfacial energies
between the adhesive material and mucus membrane and applied
mainly to liquid systems. It is the ability of a liquid to spread
spontaneously onto surface as a prerequisite for the development of
adhesion. The measure of contact angle defines the spread of liquid on
surface and as general rule the lower the contact angle, the greater
the affinity of the liquid to the solid. The spreading coefficient (SAB)
can be calculated from the surface energies of the solid and liquids
using the equation.
SAB = γB - γA - γAB
where γA is the surface tension (energy) of the liquid A, γB is the
surface energy of the solid B and γAB is the interfacial energy between
the solid and liquid. SAB should be positive for the liquid to spread
spontaneously over the solid.
The work of adhesion (WA) represents the energy required to separate
the two phases, and is given by,
WA = γA + γB - γAB.
The greater the individual surface energies of the solid and liquid,
relative to the interfacial energy, the greater the work of adhesion.
3) The adsorption theory explains the adhesion on the basis of
hydrogen bonding and van der –Waal‘s forces. It has been proposed
that these forces are the main contributors to the adhesive
interaction. A subsection of this, the chemi sorption theory, assumes
an interaction across the interface occurs as a result of strong
covalent bonding.
4) The diffusion theory laid down on the basis of the capability of
polymeric chains to diffuse across the adhesive interface. This process
is driven by concentration gradients and is dependent on the available
molecular chain lengths and their motilities. The depth of
interpenetration depends on the diffusion coefficient and the time of
contact. Sufficient depth of penetration creates a semi-permanent
adhesive bond.
5) The mechanical theory assumes that adhesion arises from an
interlocking of a liquid adhesive setting into irregularities on a rough
surface. However, rough surfaces also provide an increased surface
area available for interaction along with an enhanced visco elastic and
plastic dissipation of energy during joint failure, which are thought to
be more important in the adhesion process than a mechanical effect.
6) The fracture theory differs a little from the other defined
mechanisms in that it relates the adhesive strength to the forces
required for the detachment of the two involved surfaces after
adhesion. This assumes that the failure of the adhesive bond occurs
at the interface. However, failure normally occurs at the weakest
component, which is typically a cohesive failure within one of the
adhering surfaces.
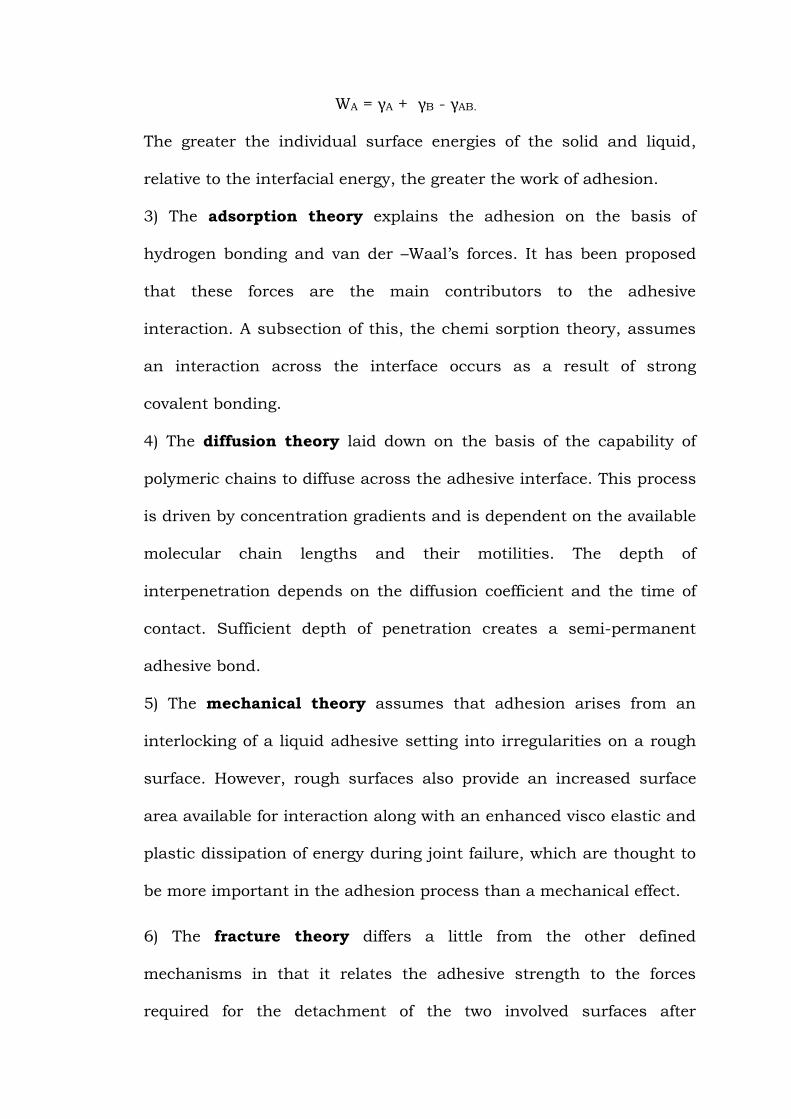
1.1.4. Process of mucoadhesion
Because of its complexity, the process of mucoadhesion cannot
be defined by just one of the above defined mechanism. By
considering the mechanism of mucoadhesion, the possible ways of
mucoadhesive bond formation in in-vivo is described as below
(Fig.1.1)
These include:
(1) Dry or partially hydrated dosage forms contacting surfaces with
substantial mucus layers (typically particulates administered into the
nasal cavity).
(2) Fully hydrated dosage forms contacting surfaces with substantial
mucus layers (typically particulates of many First Generation
mucoadhesives that have hydrated in the luminal contents on delivery
to the lower G.I. tract).
(3) Dry or partially hydrated dosage forms contacting surfaces with
thin/discontinuous mucus layers (typically tablets or patches in the
oral cavity or vagina).
(4) Fully hydrated dosage forms contacting surfaces with
thin/discontinuous mucus layers (typically aqueous semisolids or
liquids administered into the esophagus or eye).
Fig. 1.1. Some scenarios where mucoadhesion can occur in in-
vivo
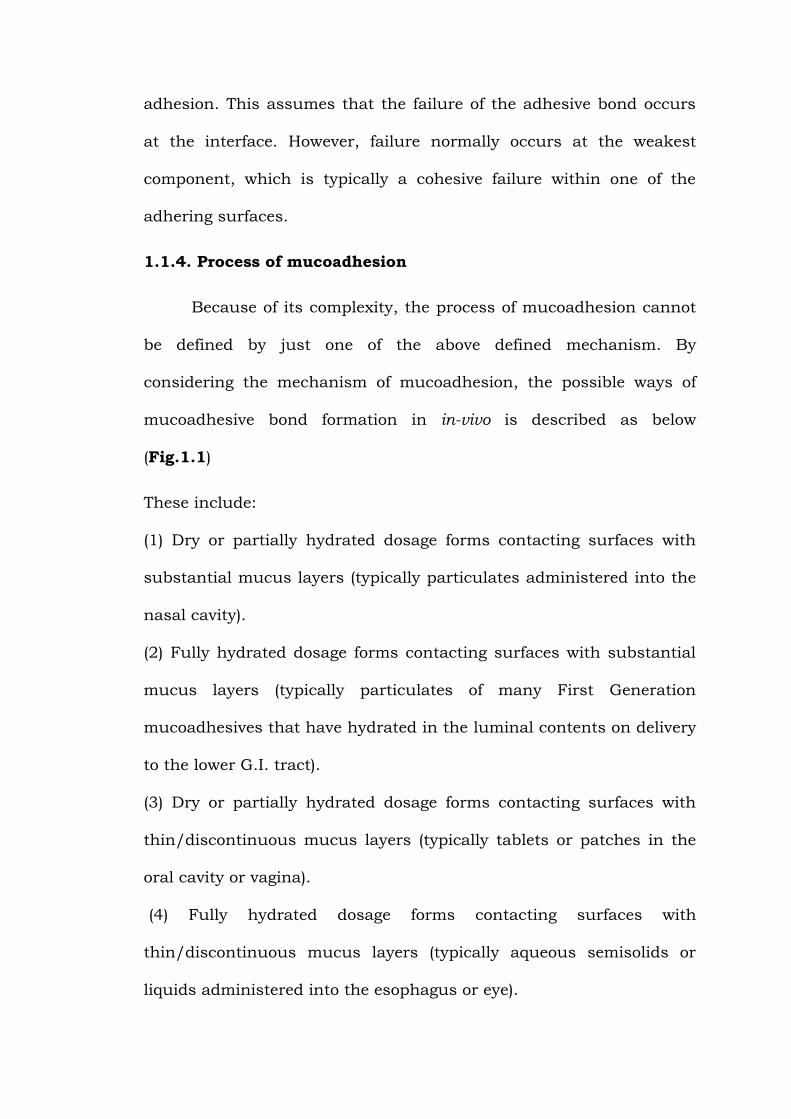
The mucoadhesive process between mucoadhesive material and a
mucus membrane takes place in two steps (Fig.1.2).
Step 1 —Contact stage: An intimate contact (wetting) occurs between
the mucoadhesive and mucous membrane.
Step 2 —Consolidation stage: Various physicochemical interactions
occur to consolidate and strengthen the adhesive joint, leading to
prolonged adhesion.
Fig 1.2: The two stages in mucoadhesion
1.1.4.1. The contact stage
The mucoadhesive and the mucous membrane have initially
come together to form an intimate contact. In some cases these two
surfaces can be mechanically brought together, e.g. placing and
holding a delivery system within the oral cavity, eye or vagina. In
others the deposition of a particle is encouraged via the aerodynamics
of the organ. For example within the nasal cavity or bronchi of the
respiratory tract deposition onto the sticky mucus coat is encouraged
by processes such as inertial impaction, in order to filter out particles
from the air stream9.
1.1.4.2. The consolidation stage
It has been proposed that if strong or prolonged adhesion is
required, a second consolidation stage is required. Mucoadhesive
materials reported to adhere most strongly to solid dry surfaces10 as
long as they are activated by the presence of moisture. Moisture will
effectively plasticize the system allowing mucoadhesive molecules to
become free, conform to the shape of the surface, and bond
predominantly by weaker van der-Waal and hydrogen bonding. In the
case of cationic materials such as chitosan, electrostatic interactions
with the negatively charged groups (such as carboxyl or sulphate) on
the mucin or cell surfaces are also possible. The mucoadhesive bond
formation is heterogeneous and is very difficult to identify, however
hydrogen bond formation is believed to be the most important. To
achieve strong adhesion, a change in the physical properties of the
mucus layer will be required otherwise it will readily fail on
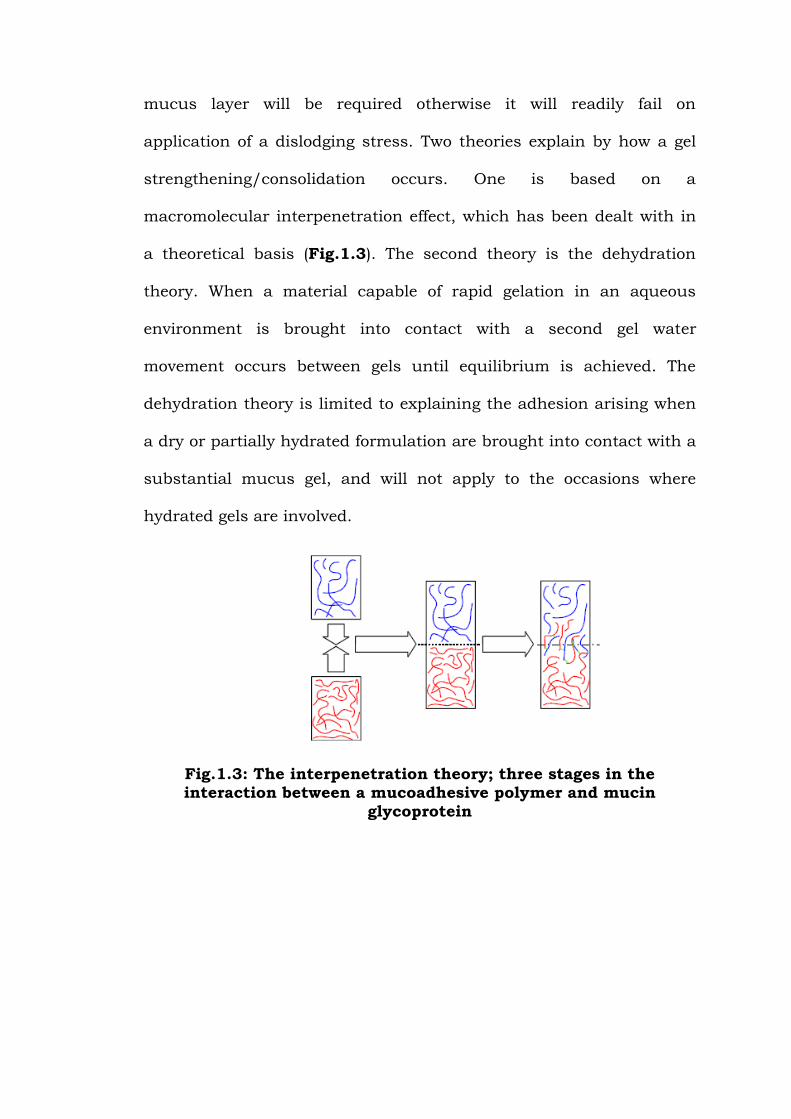
application of a dislodging stress. Two theories explain by how a gel
strengthening/consolidation occurs. One is based on a
macromolecular interpenetration effect, which has been dealt with in
a theoretical basis (Fig.1.3). The second theory is the dehydration
theory. When a material capable of rapid gelation in an aqueous
environment is brought into contact with a second gel water
movement occurs between gels until equilibrium is achieved. The
dehydration theory is limited to explaining the adhesion arising when
a dry or partially hydrated formulation are brought into contact with a
substantial mucus gel, and will not apply to the occasions where
hydrated gels are involved.
Fig.1.3: The interpenetration theory; three stages in the interaction between a mucoadhesive polymer and mucin
glycoprotein
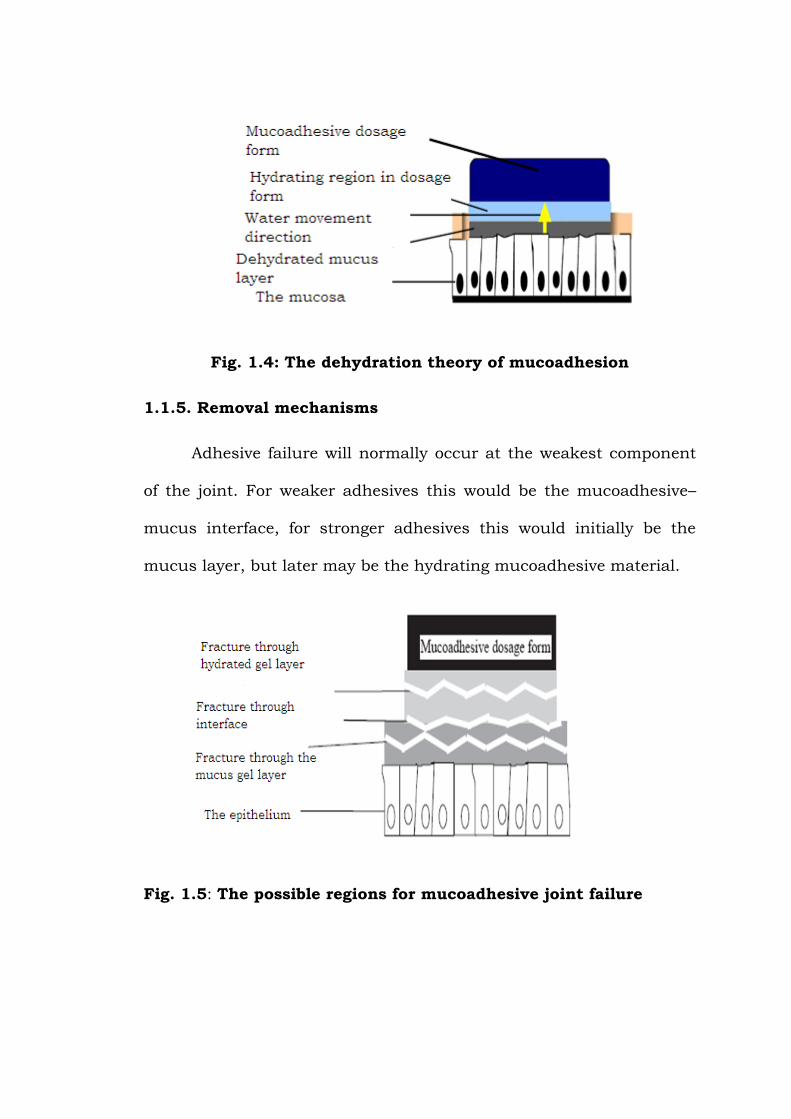
Fig. 1.4: The dehydration theory of mucoadhesion
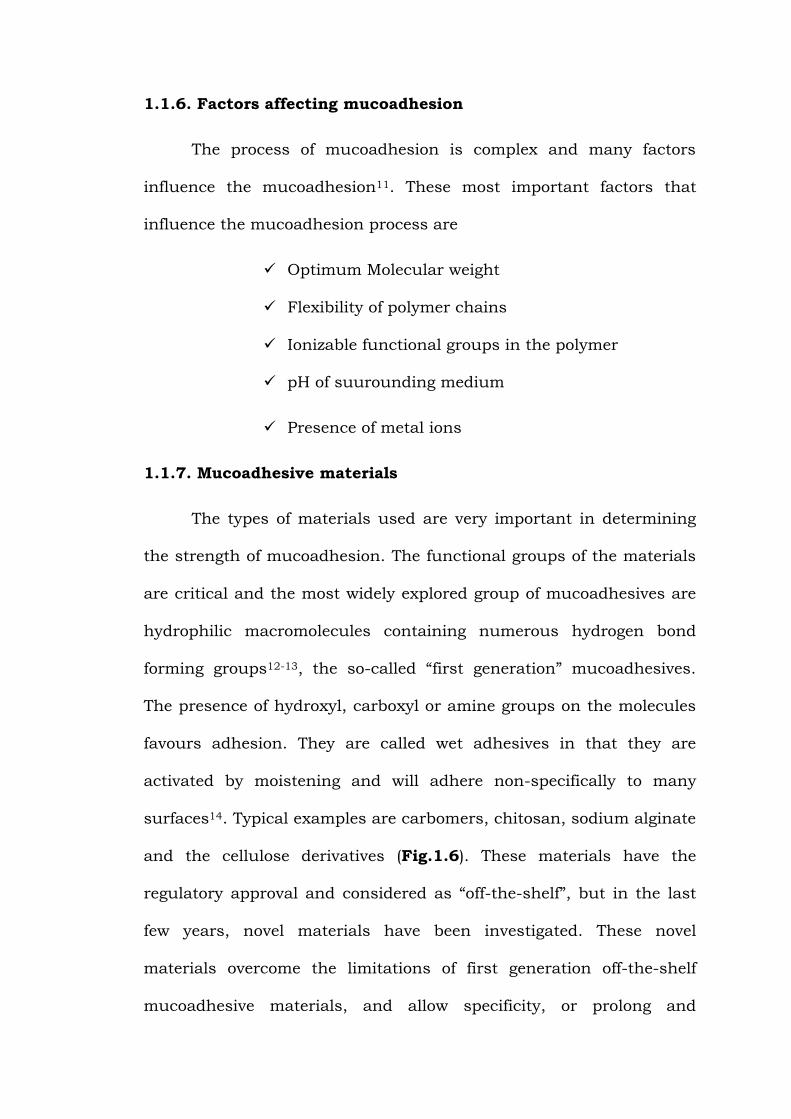
1.1.5. Removal mechanisms
Adhesive failure will normally occur at the weakest component
of the joint. For weaker adhesives this would be the mucoadhesive–
mucus interface, for stronger adhesives this would initially be the
mucus layer, but later may be the hydrating mucoadhesive material.
Fig. 1.5: The possible regions for mucoadhesive joint failure
1.1.6. Factors affecting mucoadhesion
The process of mucoadhesion is complex and many factors
influence the mucoadhesion11. These most important factors that
influence the mucoadhesion process are
Optimum Molecular weight
Flexibility of polymer chains
Ionizable functional groups in the polymer
pH of suurounding medium
Presence of metal ions
1.1.7. Mucoadhesive materials
The types of materials used are very important in determining
the strength of mucoadhesion. The functional groups of the materials
are critical and the most widely explored group of mucoadhesives are
hydrophilic macromolecules containing numerous hydrogen bond
forming groups12-13, the so-called ―first generation‖ mucoadhesives.
The presence of hydroxyl, carboxyl or amine groups on the molecules
favours adhesion. They are called wet adhesives in that they are
activated by moistening and will adhere non-specifically to many
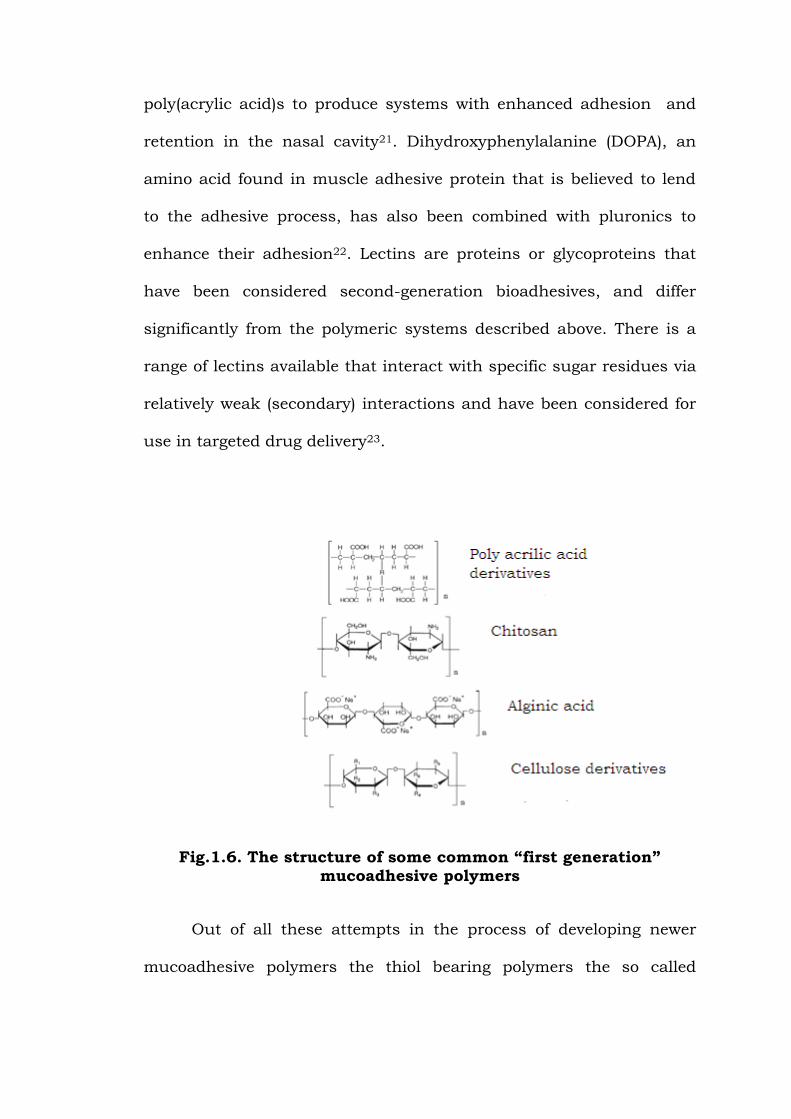
surfaces14. Typical examples are carbomers, chitosan, sodium alginate
and the cellulose derivatives (Fig.1.6). These materials have the
regulatory approval and considered as ―off-the-shelf‖, but in the last
few years, novel materials have been investigated. These novel
materials overcome the limitations of first generation off-the-shelf
mucoadhesive materials, and allow specificity, or prolong and
strengthen the mucoadhesion process. In some cases, existing
mucoadhesive polymers have been modified, while in others, new
materials are developed. One approach to produce improved
mucoadhesives has been to modify existing materials. For example
thiol groups (by coupling cysteine, thioglycolic acid, cysteamine) have
been placed into a range of mucoadhesive polymers such as the
carbomers, chitosans and alginates by Bernkop-Schnurch et al15-16.
The concept is that in-situ they will form disulphide links not only
between the polymers themselves thus inhibiting over hydration and
formation of the slippery mucilage, but also with the mucin
layer/mucosa itself, thus strengthening the adhesive joint and leading
to improved adhesive performance. This interesting approach appears
to be meeting with some success. The incorporation of ethyl hexyl
acrylate into a copolymer with acrylic acid in order to produce a more
hydrophobic and plasticized system was considered by Shojaei et al17.
The grafting of polyethylene glycol (PEG) onto poly(acrylic acid)
polymers and copolymers has also been investigated18-19. These
copolymers were shown to have favorable adhesion relative to poly
(acrylic acid) alone, in that the polyethylene glycol is proposed to
promote interpenetration with the mucus gel. Poly (acrylic acid)/PEG
complexes have also been developed as mucoadhesive materials20.
Poloxomer gels have been investigated as they are reported to show
phase transitions from liquids to mucoadhesive gels at body
temperature and will therefore allow in-situ gelation at the site of
interest. Pluronics have also been chemically combined with
poly(acrylic acid)s to produce systems with enhanced adhesion and
retention in the nasal cavity21. Dihydroxyphenylalanine (DOPA), an
amino acid found in muscle adhesive protein that is believed to lend
to the adhesive process, has also been combined with pluronics to
enhance their adhesion22. Lectins are proteins or glycoproteins that
have been considered second-generation bioadhesives, and differ
significantly from the polymeric systems described above. There is a
range of lectins available that interact with specific sugar residues via
relatively weak (secondary) interactions and have been considered for
use in targeted drug delivery23.
Fig.1.6. The structure of some common “first generation” mucoadhesive polymers
Out of all these attempts in the process of developing newer
mucoadhesive polymers the thiol bearing polymers the so called
‗Thiomers‘ have shown to be promising in the designing of new drug
delivery systems.
1.2. Thiomers
Right from the concept of mucoadhesion has arrived in the
mucoadhesive research, various attempts have been undertaken in
order to improve the adhesive properties of polymers. These
approaches include the use of linear poly(ethylene glycol) as adhesion
promoter for hydrogels, the neutralization of ionic polymers,
mucoadhesion by a sustained hydration process and the development
of polymer–adhesion conjugates providing a specific binding to
epithelia. However, all these systems are based on the formation of
non-covalent bonds such as hydrogen bonds, van der-Waal‘s forces,
and ionic interactions. Accordingly, they ended with a relatively weak
mucoadhesion, in many times failed in the localization of a drug
delivery system at a given target site for longer duration of time.
Mucoadhesive polymers have therefore in many cases not proven to be
effective as pharmaceutical glue. In the process of identifying novel
mucoadhesive excipients a presumptive new generation of
mucoadhesive polymers, thiolated polymers—designated thiomers,
were discovered24. In contrast to well-established mucoadhesive
polymers these novel polymers are capable of forming covalent bonds.
These thiomers creates a disulfide bond with biological systems
thereby been discovered for the covalent adhesion of polymers to the
mucus gel layer of the mucosa. Thiomers are mucoadhesive basis
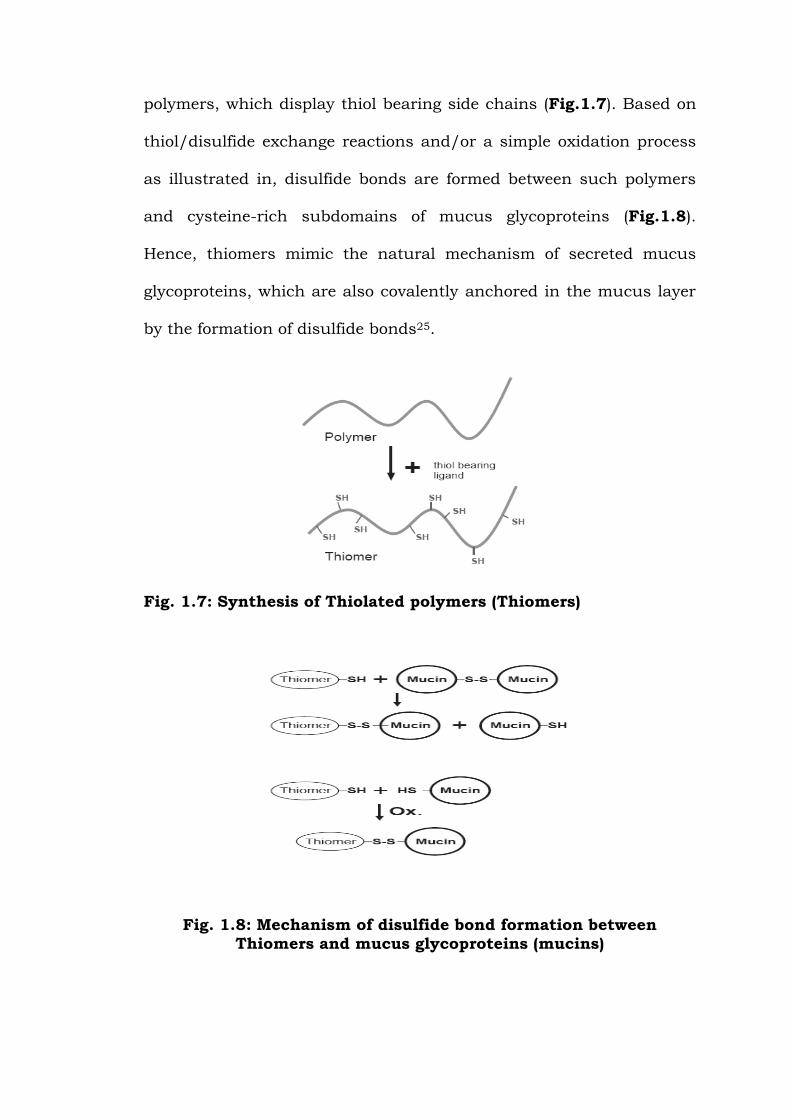
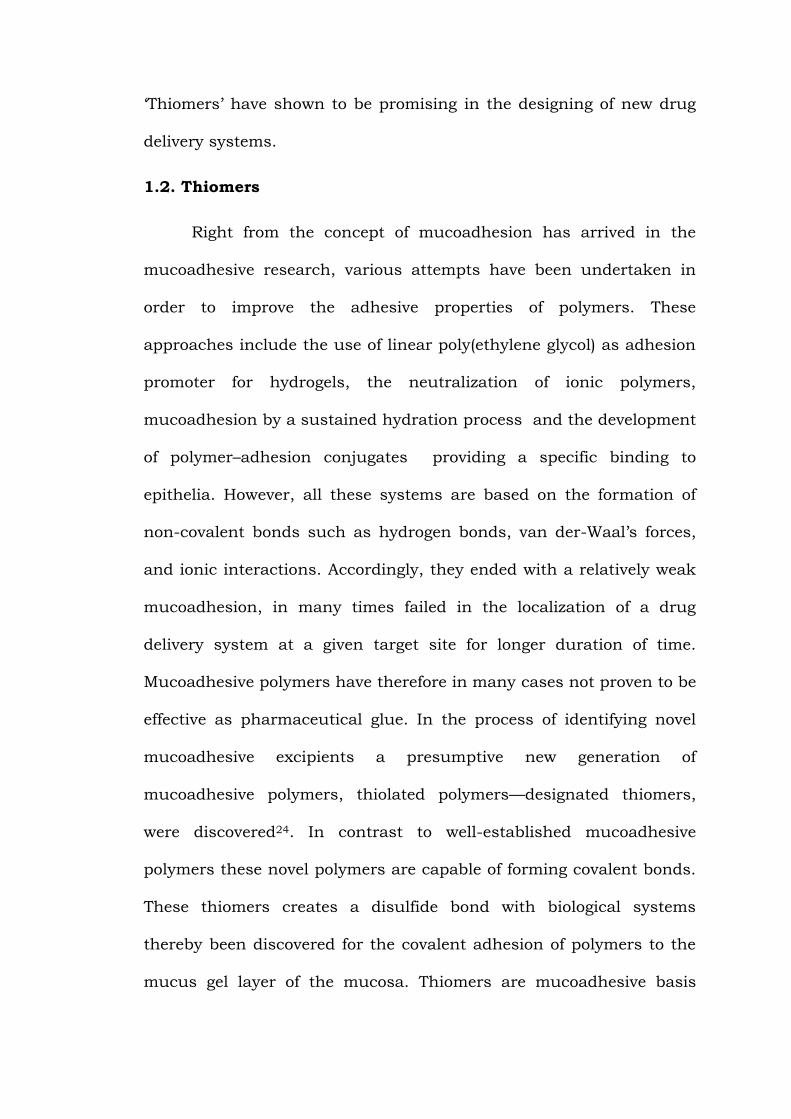
polymers, which display thiol bearing side chains (Fig.1.7). Based on
thiol/disulfide exchange reactions and/or a simple oxidation process
as illustrated in, disulfide bonds are formed between such polymers
and cysteine-rich subdomains of mucus glycoproteins (Fig.1.8).
Hence, thiomers mimic the natural mechanism of secreted mucus
glycoproteins, which are also covalently anchored in the mucus layer
by the formation of disulfide bonds25.
Fig. 1.7: Synthesis of Thiolated polymers (Thiomers)
Fig. 1.8: Mechanism of disulfide bond formation between
Thiomers and mucus glycoproteins (mucins)
1.2.1. Types of Thiomers
Based on the surface functional groups generated on the
polymers thiomers are classified into cationic thiomers and anionic
thiomers.
1.2.1.1. Cationic thiomers
Cationic thiomers mainly exhibits primary amino group as
anionic substrate. Chiotsans are widely studied substance in the
preparation of cationic thiomers. The primary amino group at the 2-
position of the glucosamine subunits of this polymer is the main
target for the immobilization of thiol groups. Various carboxylic acid
group containing ligands such as cysteine and thioglycolic acid can
be covalently attached to this primary amino group via the formation
of amide or amidine bonds. These carboxylic groups react with amine
groups of chitosan mediated for instance by carbodiimides. An
unintended oxidation of thiol groups during synthesis can be avoided
by performing the reaction under inert conditions or at controlled pH
conditions. Furthermore, disulfide bonds can be reduced after the
synthesis process by the addition of reducing agents such as
dithiotreithol or borohydride. 2-Iminothiolane is also can be used as
coupling agent to attach by amidine bonds 2-iminothiolane. It offers
the advantage of a simple one step coupling reaction. In addition, the
thiol group of the reagent is protected towards oxidation due to its
chemical structure26.
1.2.1.2. Anionic thiomers
Anionic thiolated polymers represent the presence of anionic
substructures on the polymer surface such as carboxylic groups.
These carboxylic acid groups can be easily attached to polymers
through the formation of amide bonds. Sulfahydral bearing ligands
such as cysteine, cysteamine and homocysteine are used. The
formation of amide bonds can be mediated by carbodiimides. The
formation of oxidative products can be minimized by conducting the
reaction at controlled conditions. In addition, disulfide bonds formed
during synthesis can be cleaved thereafter by the addition of reducing
agents such as dithiothreitol or NaBH4.
1.2.2. Mechanisms for improved mucoadhesion by thiomers
The formation of disulfide bonds between the thiomers and the
mucus gel layer takes place either via thiol/disulfide exchange
reactions or via a simple oxidation process of free thiol groups.
Generally there are no mucosal surfaces in which mucins with
cysteine rich subdomains are not present. In contrast to noncovalent
bonds disulfide bonds are not influenced by factors such as ionic
strength and pH. Velocity and extent of disulfide bond formation
depends on the concentration of thiolate anions representing the
reactive form for thiol/disulfide exchange reactions and oxidation
processes. The concentration of thiolated anions in turn depends on:
a) The pKa value of the thiol group in dependence on the polymer
backbone and the chemical structure of the ligand, more or less
reactive thiomers can be designed. Thiol groups of the chitosan–
thiobutylamidine conjugate, for instance, exhibit a pKa value of 9.9,
whereas the pKa value of the thiol groups of poly(acrylate)–cysteine
conjugates is 8.35.
b) The pH of the thiomer. As only ionic thiomers are used, they all
display a high buffer capacity. The buffer capacity of a sodium
poly(acrylate) matrix tablet, for instance, can be compared with that of
an at least 25 M acetate buffer. As all charged groups remain
concentrated on the polymeric network a kind of ―microclimate‖ can
be established. The reactivity of thiol groups can consequently be
controlled by adjusting the pH of the polymer to a certain level. The
higher the pH is adjusted, the more reactive are the thiol groups and
vice versa
c) And the pH of the surrounding medium. The reactivity of thiol
groups inside the polymeric network is mainly controlled by the pH of
the thiomer, whereas the reactivity on the surface of the polymer is
more controlled by the pH of the surrounding medium. As the mucus
gel layer being close to the epithelium has a pH around 7, thiol groups
penetrating into the mucus are always sufficiently reactive. Leitner et
al27 could show by four different methods including rheological,
diffusion, gel permeation and certain mucoadhesion studies the
formation of disulfide bonds between thiolated polymers and mucus
glycoproteins.
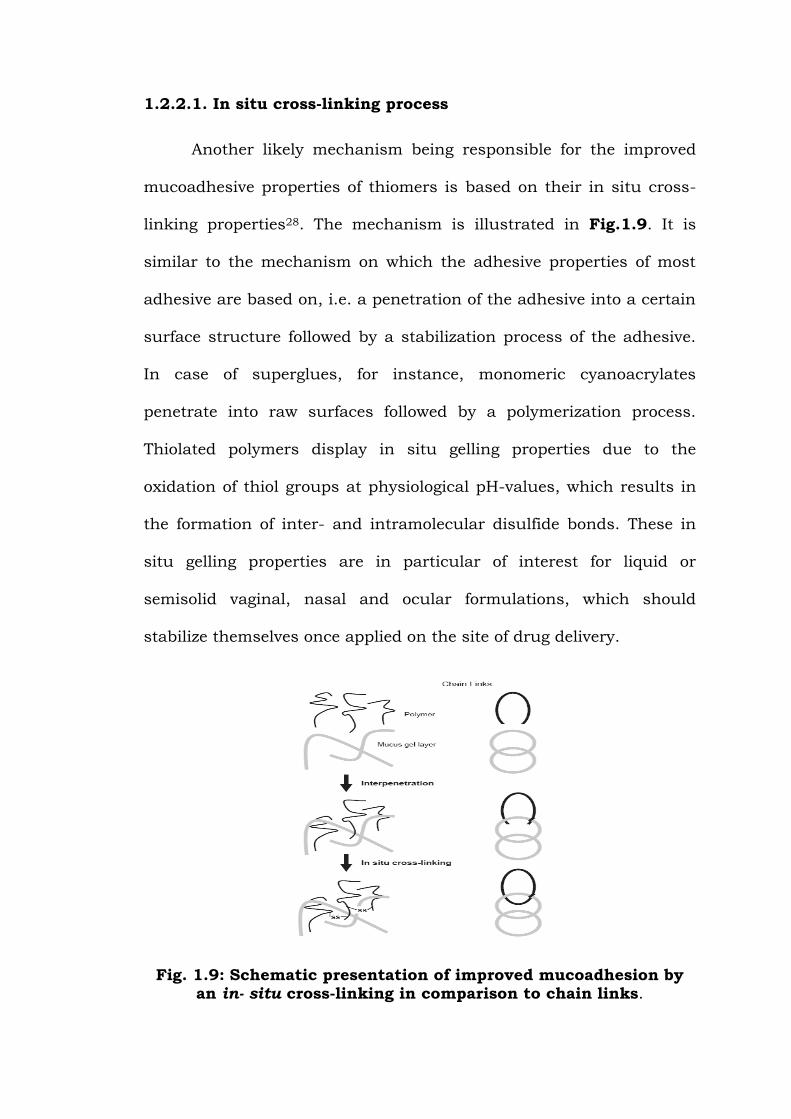
1.2.2.1. In situ cross-linking process
Another likely mechanism being responsible for the improved
mucoadhesive properties of thiomers is based on their in situ cross-
linking properties28. The mechanism is illustrated in Fig.1.9. It is
similar to the mechanism on which the adhesive properties of most
adhesive are based on, i.e. a penetration of the adhesive into a certain
surface structure followed by a stabilization process of the adhesive.
In case of superglues, for instance, monomeric cyanoacrylates
penetrate into raw surfaces followed by a polymerization process.
Thiolated polymers display in situ gelling properties due to the
oxidation of thiol groups at physiological pH-values, which results in
the formation of inter- and intramolecular disulfide bonds. These in
situ gelling properties are in particular of interest for liquid or
semisolid vaginal, nasal and ocular formulations, which should
stabilize themselves once applied on the site of drug delivery.
Fig. 1.9: Schematic presentation of improved mucoadhesion by an in- situ cross-linking in comparison to chain links.
1.2.3. Features of thiomers
The thiomers because of its surface bearing sulfahydral groups
and its polymeric nature, they exhibit different properties and found
to be advantageous for variety of applications. These include
Mucoadhesive and cohesive properties29-30
Enzyme inhibitory properties30-31
Permeation enhancing properties32-33
Thiomers as matrices for controlled drug release34
1.2.4. Stability of thiomers
Because of the sensitivity of thiol groups towards oxidation, the
chemical stability of thiomers has already been investigated in detail.
PCP-Cys and chitosan-TGA were tested both as representative anionic
and cationic candidates, respectively. And found to be stable under all
storage conditions when compressed into matrix tablets35.
With the introductory note above described about the
advantages of mucoadhesive systems and applications of thiomers, it
is concluded that the potential of thiomeric mucoadhesive drug
delivery systems for the designing of formulations for small molecule
drugs, proteins and peptides for various routes of administration is
enormous, however so far synthesized thiomers have limited
sulfahydral groups and the resultant mucoadhesion is weak. For
producing the longer mucoadhesion with the same thiomers require
larger quantity of polymer which is an inhibiting factor. And some
polymers are of carbohydrate based and may be antigenic. The
polymers which are having multiple reactive functional groups to
conjugate with thiol bearing ligands, biocompatible, non antigenic will
be of advantage in preparing the thiomeric polymers. Dendrimers with
its multiple surface functional groups are suitable for synthesizing the
thiomers with high amount of thiol per mole of dendrimer.
1.3. Dendrimers
As polymer science has evolved over the past two centuries, the
number of compositions and architectures of macromolecules
synthetically accessible has also grown. The ability to easily tune the
size, chemistry, topology and ultimately the properties of polymers
through chemical synthesis inevitably has led to their widespread use
in variety of technological applications. The myriad properties and
functions that can be designed into polymeric systems are prompting
the medical community to use polymers in the drug delivery, tissue
engineering and biological imaging. The highly branched and
symmetrical molecules as dendrimers are the most recently
recognized members of the polymer family, with the first dendrimer
reports published in the late 1970s and early 1980s by the several
groups36-39. Dendritic polymers can differ significantly from linear
polymers in their properties. They have a number of beneficial
attributes for biomedical applications, including the following:
Bio distribution and pharmacokinetic properties that can be
tuned by controlling dendrimer size and conformation. This can
be achieved with precision by varying dendrimer generation
number or by creating dendrimer-polymer hybrids.
Huge structural and chemical homogeneity, dendrimer
biological properties can be attributable to a single molecular
entity and not a statistical distribution of polymeric or self
assembled materials facilitating the reproducibility of
pharmacokinetic data within and between different synthetic
loss.
Ability to be functionalized with multiple copies of drugs,
chromophores or ligands either at their peripheries and/or their
interiors. Dendrons also can be used to precisely increase the
drug loading capacity of carriers, such as antibodies and
biocompatibility polymers like poly(ethylene glycol).
High ligand density, unlike in linear polymers as dendrimer‘s
generation increases, the multivalent ligand density at the
surface increases, which can strength ligand receptor binding
and improve the targeting of attached components.
Controlled degradation: This can be achieved by judicious
choice of dendrimer chemistry, with unique modes of
decomposition accessible through use of self immolative
dendrimers.
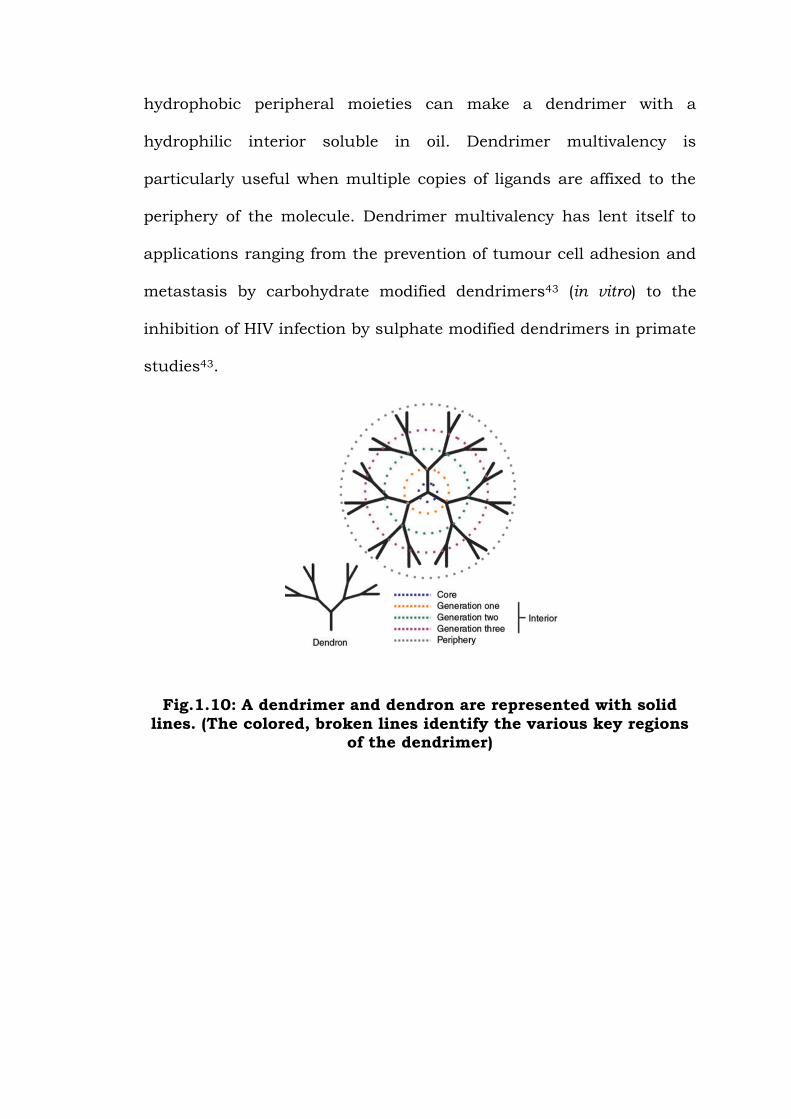
1.3.1. Dendrimer chemistry and structure
A dendrimer is a polymeric molecule composed of multiple
perfectly branched monomers that emanate radially from a central
core reminiscent of a tree, hence dendrimers derive their name (Greek
Dendra). A dendron can be divided into three different regions: The
core, the interior (or branches) and the periphery (or end groups). The
number of branch points encountered upon moving outward from the
core of the dendron to its periphery defines its generation (G-1, G-2,
G-3), dendrimers of higher generations are larger, more branched and
have more end groups at their periphery than dendrimers of lower
generations (Fig.1.10). A dendrimer may be based on practically any
type of chemistry, the nature of which can determine its solubility,
degradability and biological activity. Some of the commonly
encountered types of dendrimers in biological applications are based
on polyamidoamines40, polyamines41, polyamides (polypeptides),
poly(aryl ethers), polyesters, carbohydrates and DNA42 (Fig 1.11). By
far the most common dendrimer scaffold is that of the
polyamidoamine (PAMAM) dendrimers, which are available
commercially with a wide variety of generation and peripheral
functionalities.
Perhaps the most exploited property of dendrimers is their
multivalency. Unlike in linear polymers, as dendrimer molecular
weight and generation increases, the terminal units become more
closely packed, a feature exploited by many investigators as a means
to achieve concentrated payloads of drugs or spectroscopic labels for
therapeutic and imaging applications. The many end groups can also
greatly modulate dendrimers solubility: hydrophilic end groups can
make water soluble a dendrimer with a hydrophobic core; where as
hydrophobic peripheral moieties can make a dendrimer with a
hydrophilic interior soluble in oil. Dendrimer multivalency is
particularly useful when multiple copies of ligands are affixed to the
periphery of the molecule. Dendrimer multivalency has lent itself to
applications ranging from the prevention of tumour cell adhesion and
metastasis by carbohydrate modified dendrimers43 (in vitro) to the
inhibition of HIV infection by sulphate modified dendrimers in primate
studies43.
Fig.1.10: A dendrimer and dendron are represented with solid
lines. (The colored, broken lines identify the various key regions of the dendrimer)
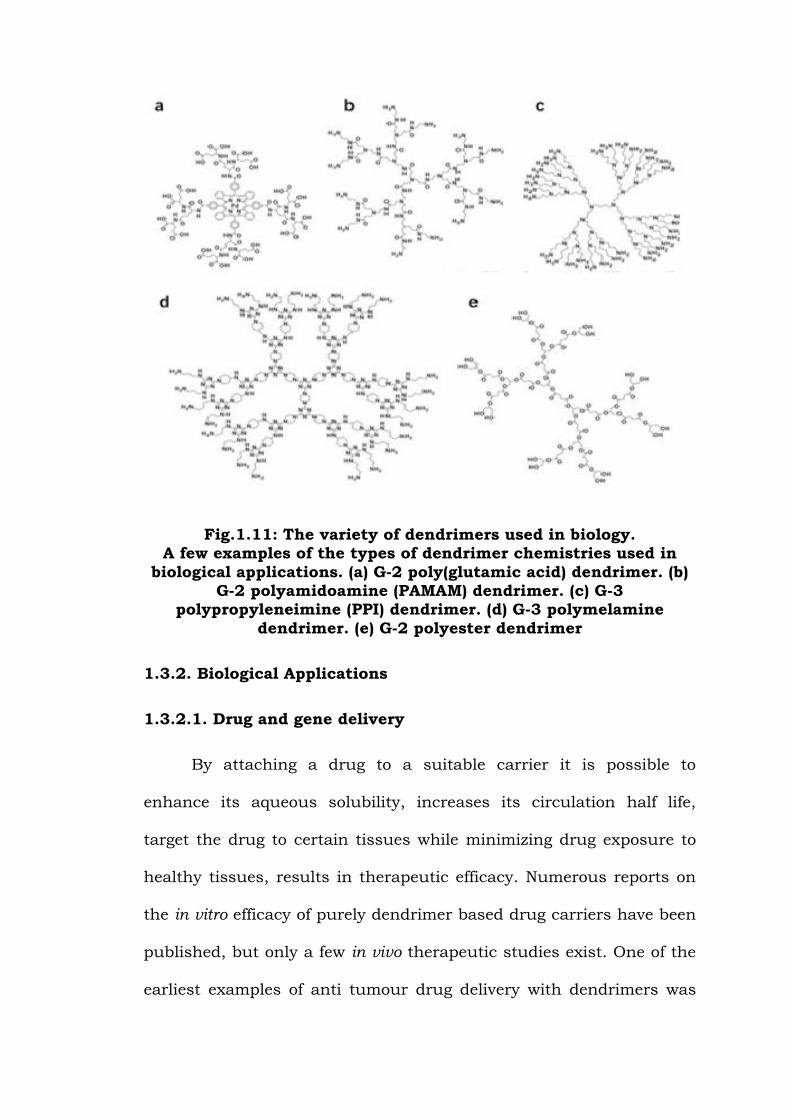
Fig.1.11: The variety of dendrimers used in biology. A few examples of the types of dendrimer chemistries used in
biological applications. (a) G-2 poly(glutamic acid) dendrimer. (b) G-2 polyamidoamine (PAMAM) dendrimer. (c) G-3
polypropyleneimine (PPI) dendrimer. (d) G-3 polymelamine
dendrimer. (e) G-2 polyester dendrimer
1.3.2. Biological Applications
1.3.2.1. Drug and gene delivery
By attaching a drug to a suitable carrier it is possible to
enhance its aqueous solubility, increases its circulation half life,
target the drug to certain tissues while minimizing drug exposure to
healthy tissues, results in therapeutic efficacy. Numerous reports on
the in vitro efficacy of purely dendrimer based drug carriers have been
published, but only a few in vivo therapeutic studies exist. One of the
earliest examples of anti tumour drug delivery with dendrimers was
achieved by complexing cisplatin (20-25% by weight) to the surface
groups of G-4 carboxylate terminated PAMAM dendrimer45.
Conjugation of cisplatin to the dendrimer led to a tenfold increase in
cisplatin solubility, but the drug also caused cross linking between
dendrimers, resulting in aggregates with diameters 3-40 nm. When
administered intravenously to mice, the aggregates targeted
subcutaneous tumours via a passive targeting mechanism known as
the enhanced permeation and retention effect. PAMAM dendrimers
have also been used as anti tumour targeted carriers of
methotrexate46. The peripheral amines of G-5 PAMAM dendrimers
were first partially modified with acetyl groups to reduce dendrimer
surface charge. The acetylated PAMAM was subsequently
functionalized with folate as a targeting ligand.
1.3.2.2. Imaging
In vivo imaging is an increasingly useful tool in biomedicine, as
it is non-invasive and provides a wealth of information regarding the
native states of a variety of tissue types. The earliest in vivo uses of
dendrimers were as carriers for magnetic resonance imaging contrast
reagents47. Another non invasive imaging application of dendrimers
involves photonic oxygen sensing. By encapsulating hydrophobic
metalloporphyrins in the cores of variously sized poly (glutamic acid),
poly (aryl ether) or poly (ether amide) dendrimers Vinogradov et al48
have prepared water soluble oxygen sensors whose phosphorescence
is quenched upon collision with dissolved oxygen.
1.3.2.3. Intrinsic drug properties
Whereas the majority of dendrimer designs have been used as
carriers for drugs and nucleic acids, some dendrimers act as drugs
themselves. Supattapone et al49 discovered that branched polyamines
including PAMAM dendrimers and hyper branched polymers stimulate
the removal of prion proteins present in infected cells. The branched
architecture appears essential to this application because linear
polyamines and small molecule amines are ineffective.
Multivalent display of ligands on the surface of a dendrimer has
also proven to be a viable method of inhibiting multivalent binding
between cells, viruses, bacteria, proteins and combinations thereof.
For example, a G-4 poly(L-Lysine) dendrimer bearing sulphate groups
at its periphery is being evaluated as an anti viral topical ointment50.
1.3.3. Biocompatibility of dendrimers
The success of dendrimers as carriers or biomaterials will
depend in large part on their biocompatibility-whether dendrimers
elicit an undesirable response from their biological host. Long term
accumulation of low molecular weight compounds is not often a
problem because they are excreted in the urine or in the faeces after
metabolism. However, injected polymers are not eliminated as easily,
especially if they are not readily degraded into smaller units51 or are
too large to be filtered via the kidneys. Thus for dendrimers which can
be classified as low molecular weight or polymeric depending on their
generation, acceptable biocompatibility must be accompanied by a
reasonably fast renal elimination rate or biodegradation rate.
1.3.3.1. In vitro toxicity
In most cases, the nature of a dendrimers numerous end
groups dictate whether or not it displays significant toxicity. For
example, cationic dendrimers with terminal primary amino groups
such as PAMAM and polypropyleneimine (PPI) dendrimers generally
display concentration dependent toxicity and haemolysis52, where as
dendrimers containing only neutral or anionic components have been
shown to be much less toxic and less haemolytic. Cytotoxicity of
amino terminated dendrimers can be lessened by partial or complete
modification of the dendrimer periphery with negatively charged or
neutral groups53. The toxicity of cationic PAMAM dendrimers with
each generation, but surprisingly cationic PPI dendrimers does not
follow this trend.
1.3.3.2. In vivo toxicity
In vivo toxicity correlates reasonably well with in vitro toxicity.
Mice tolerate low intraperitoneal doses of positively charged PAMAM
dendrimers (~ 10 mg/kg). Acute and sub chronic toxicity studies in
mice with melamine dendrimers bearing cationic surface charges
revealed that intraperitoneally administered doses above 10 mg/kg
produced liver toxicity, as demonstrated by increased levels of alanine
transaminase in serum and liver necrosis upon histopathological
analysis. When ~ 50 % of the cationic groups of a structurally similar
dendrimer were replaced with neutral polyethylene oxide chains, no
acute or sub chronic toxicity was observed after intraperotoneal of
intravenous injection of doses greater than 1 g/kg54, similarly, a
family of non charged polyester dendrimer showed very low toxicity.
1.3.4. Degradation behavior of dendrimers
Biodegradability of dendrimers is a valuable attribute that can
prevent bioaccumulation and the possible toxic effects associated with
its occurrence. The most widely studied dendrimers, PAMAMs, are
hydrolytically degradable only under harsh conditions because of their
amide backbones and hydrolysis proceeds slowly at physiological
temperatures. Photolytically labile dendrimers may allow external
initiator and spatially addressable dendrimer degradation. Dendrimers
in which the dendrons are released from the core in which the
dendrimer peripheral groups are cleaved55 or in which the dendrimer
peripheral groups are cleaved or in which the entire dendrimer
degrades into a identical small molecule fragments upon ultraviolet
irradiation have been prepared. Although the aromatic decompositions
products of some of the dendrimers are non-toxic. It will be interesting
to earn if less hydrophobic aliphatic molecules cab be used to increase
dendrimer solubility and ensure their biocompatibility.
1.3.5. Pharmacokinetics behavior of dendrimers
An understanding of dendrimer pharmacokinetics is essential
for their application in medicine because the bioavailability, toxicity
and ultimately efficacy of dendrimer based drugs and imaging agents
will depend on heir tissue accumulation profiles, drug release rates
and elimination rates56. The important feature is he that drugs that
are loaded into dendrimers using non covalent hydrophobic or
hydrogen bonding interactions are rapidly released when the
dendrimer drug combination is placed into the bio phase and thus
drug targeting is not optimal because the drug leaves the carrier
before the carrier arrives at its intended target.
In the view of above described advantages of dendrimers here in
the present project it is decided to prepare novel thiolated dendrimer
excipients for designing the mucoadhesive systems. Hence by virtue of
combining the advantages of thiomers in mucoadhesion and
dendrimers in mucosal penetration behavior the prepared thiolated
dendrimers will be tested for their efficacy by applying to different
mucosal organs such as ocular, oral and nasal.
1.4. Ocular delivery
Topical administration of therapeutic moieties to the eye is the
most popular and well recognized route of administration for the
treatment of ocular disorders. However, because of efficient protective
mechanisms of the eye, such as blinking, baseline and reflex
lachrymation and drainage remove rapidly foreign substances,
including drugs, from the surface of the eye, the ocular formulations
are rapidly drained from the ocular surface and limits the
bioavailability only to below 5% and also the residence time of the
formulation is very short57. Moreover, the anatomy, physiology and
barrier function of the cornea compromise the rapid absorption of
drugs58. In order to achieve the therapeutic levels of drugs, frequent
dosage of formulations is required but it may result in inducing toxic
side effects and cellular damage at the ocular surface59-60. To improve
the ocular bioavailability and penetration, the applied formulations
shall contact the cul-de-sac for prolonged time. Various strategies
have been developed and met some success in meeting the
therapeutic efficacy.
1.4.1. Anatomy and physiology of eye
The structure and construction of eye is very complex. The
protective wall of the eyeball has consists of three layers: the outer
coat or the sclera and cornea, a middle layer or uveal coat and the
inner coat or retina. The sclera is made of fibrous tissues shaped as
segments of two spheres, the sclera and cornea61. The external part of
the eye is covered by the mobile tarsal part of the eyelids. The eyelids
are under involuntary and voluntary control. They play role in
distributing the tear fluid over the eye, providing an optically smooth
surface over the cornea. The shear rate during blinking is estimated to
be about 20,000 s_1, and influences ocular bioavailability of applied
drugs by influencing the rheological properties62.
The cornea is a clear, transparent, avascular tissue to which
nutrients and oxygen are supplied by the lachrymal fluid and aqueous
humour. It is composed of five layers: epithelium, Bowman‘s layer,
stroma, Descemet‘s membrane and endothelium
The conjunctiva is a thin transparent membrane, which lines
the inner surface of the eyelids and is reflected onto the globe. At the
corneal margin, it is structurally continuous with the corneal
epithelium. The membrane is vascular and moistened by the tear film.
The conjunctiva is composed of an epithelium, a highly vascularised
substantia propria, and a submucosa or episclera. The bulbar
epithelium consists of 5 to 7 cell layers. At the surface, epithelial cells
are connected by tight junctions, which makes the conjunctiva
relatively impermeable. The conjunctival tissue is permeable to
molecules up to 20,000 Da, whereas the cornea is impermeable to
molecules larger than 5000 Da.
The mucus layer is very sensitive to hydration and forms a gel-
layer with viscoelastic rheological properties. It protects the epithelia
from damage and facilitates the movements of the eyelids. Mucins
improve the spreading of the tear film and enhance its stability and
cohesion. Mucus is wiped over the surface of the eye by the upper
eyelid during blinking. The mucus gel entraps bacteria, cell debris,
and foreign bodies, forming mucous threads consisting of thick fibers
arranged in bundles. These threads are transported during blinking to
the inner canthus and expelled onto the skin. The mucus layer can
form a diffusion barrier to macromolecules depending on the degree of
network entanglement. On the other hand, mucus can bind cationic
substances because of the negative charges of mucins. Mucus
consists of glycoproteins, proteins, lipids, electrolytes, enzymes, muco
polysacchrides and water. The primary component of mucus is mucin,
a high-molecular-mass glycoprotein with subunits containing a
protein core, approximately 800 amino acids long, of which about 200
are bearing polysaccharide side-chains. The protein core consists of
tandem repeat regions, which are repeated sequences of mainly
serine, threonine and proline. The polysaccharide side chains are
linked to the protein core by an O-glycosidic bond between N-
acetylgalactosamine on the sugar chain and the hydroxyl groups of
the serine and threonine residues on the protein backbone. As the
polysaccharide side chains usually terminate in either fucose or sialic
acid (N-acetylneuraminic acid, pKa=2.6), the glycoprotein is negatively
charged at physiological pH.
1.4.2. Ocular Pharmacokinetics
The main routes of drug administration and elimination from
the eye have been shown schematically in the below figure (Fig. 1.12).
They are
1) Transcorneal permeation from the lacrimal fluid into the
anterior chamber.
2) Non-corneal drug permeation across the conjunctiva and sclera
into the anterior uvea
3) Drug distribution from the blood stream via blood-aqueous
barrier into the anterior chamber
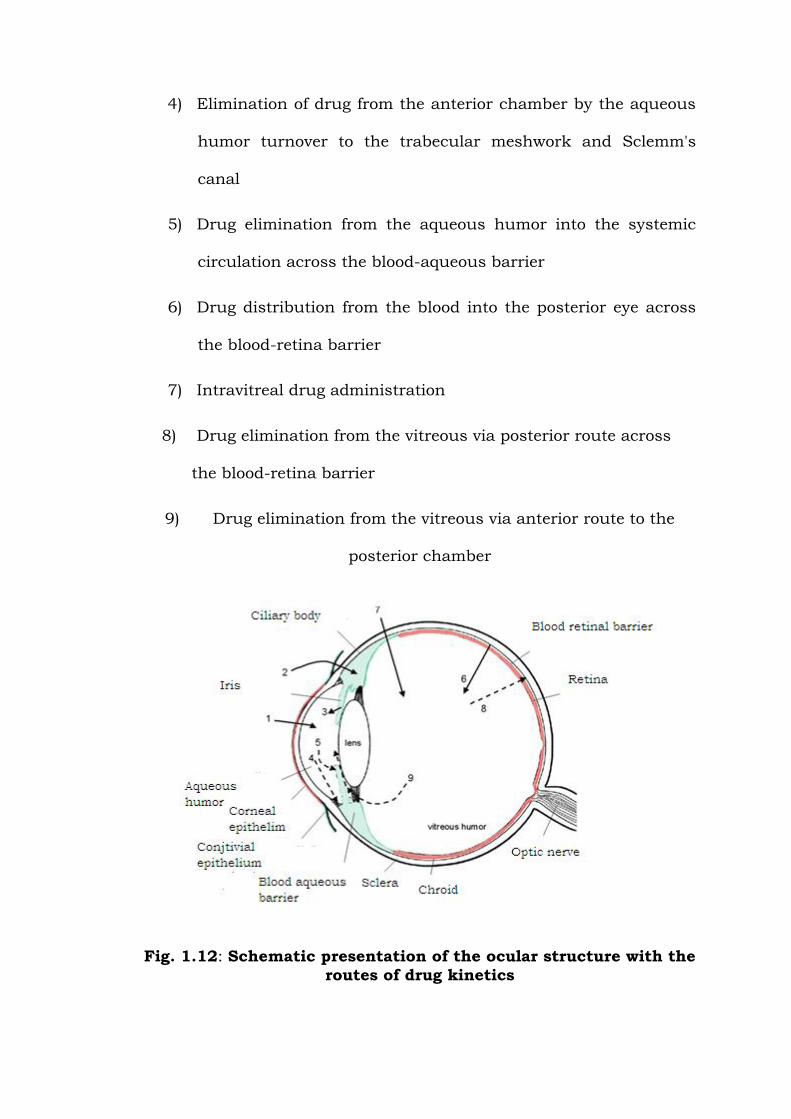
4) Elimination of drug from the anterior chamber by the aqueous
humor turnover to the trabecular meshwork and Sclemm's
canal
5) Drug elimination from the aqueous humor into the systemic
circulation across the blood-aqueous barrier
6) Drug distribution from the blood into the posterior eye across
the blood-retina barrier
7) Intravitreal drug administration
8) Drug elimination from the vitreous via posterior route across
the blood-retina barrier
9) Drug elimination from the vitreous via anterior route to the
posterior chamber
Fig. 1.12: Schematic presentation of the ocular structure with the
routes of drug kinetics
1.4.3. The barriers for corneal absorption of drugs
a) Drug loss from the ocular surface
After administration, the flow of lacrimal fluid removes the
therapeutic agents from the surface of the eye. After application the
dosage form, the excess volume is cleared from nasolacrimal duct63.
Another way of drug removal from ocular surface is by systemic
absorption through conjunctival sac or through nasal cavity64.
b) Lacrimal fluid-eye barriers
Another barrier which prevents the drug absorption from
corneal epithelium is the lacrimal fluid. The corneal barrier is formed
upon maturation of the epithelial cells. They migrate from the limbal
region towards the center of the cornea and to the apical surface. The
most apical corneal epithelial cells form tight junctions that limit the
paracellular drug permeation65. Hence, lipophilic drugs have
increased permeability than the hydrophilic drugs. Despite the
tightness of the corneal epithelial layer, transcorneal permeation is
the main route of drug entrance from the lacrimal fluid to the aqueous
humor. It is considered that, the conjunctiva is more leaky epithelium
than the cornea and its surface area is also nearly 20 times greater
than that of the cornea.
c) Blood-ocular barriers
The eye is protected from the forgein matter in the blood stream
by blood-ocular barriers. These barriers have two parts: blood-
aqueous barrier and blood-retina barrier. The anterior blood-eye
barrier is composed of the endothelial cells in the uvea. This barrier
prevents the access of plasma albumin into the aqueous humor, and
also limits the entry of hydrophilic drugs from plasma into the
aqueous humor. The posterior barrier between blood stream and eye
is comprised of retinal pigment epithelium (RPE) and the tight walls of
retinal capillaries. Unlike retinal capillaries the vasculature of the
choroid has extensive blood flow and leaky walls. Drugs easily gain
access to the choroidal extravascular space, but thereafter
distribution into the retina is limited by the RPE and retinal
endothelia. Despite its high blood flow the choroidal blood flow
constitutes only a minor fraction of the entire blood flow in the body.
Therefore, without specific targeting systems only a minute fraction of
the intravenous or oral drug dose gains access to the retina and
choroid. Unlike blood brain barrier, the blood-eye barriers have not
been characterised in terms of drug transporter and metabolic enzyme
expression.
1.4.5. Drug elimination from lacrimal fluid
Several mechanisms such as a relatively impermeable cornea1
barrier and rapid drainage of the instilled solution protect the eye.
Mechanistic studies by Lee and Robinson66 have shown that drugs are
mainly eliminated from the pre corneal lacrimal fluid by solution
drainage, lacrimation and nonproductive absorption to the
conjunctiva of the eye (Fig. 1.13). These factors and the cornea1
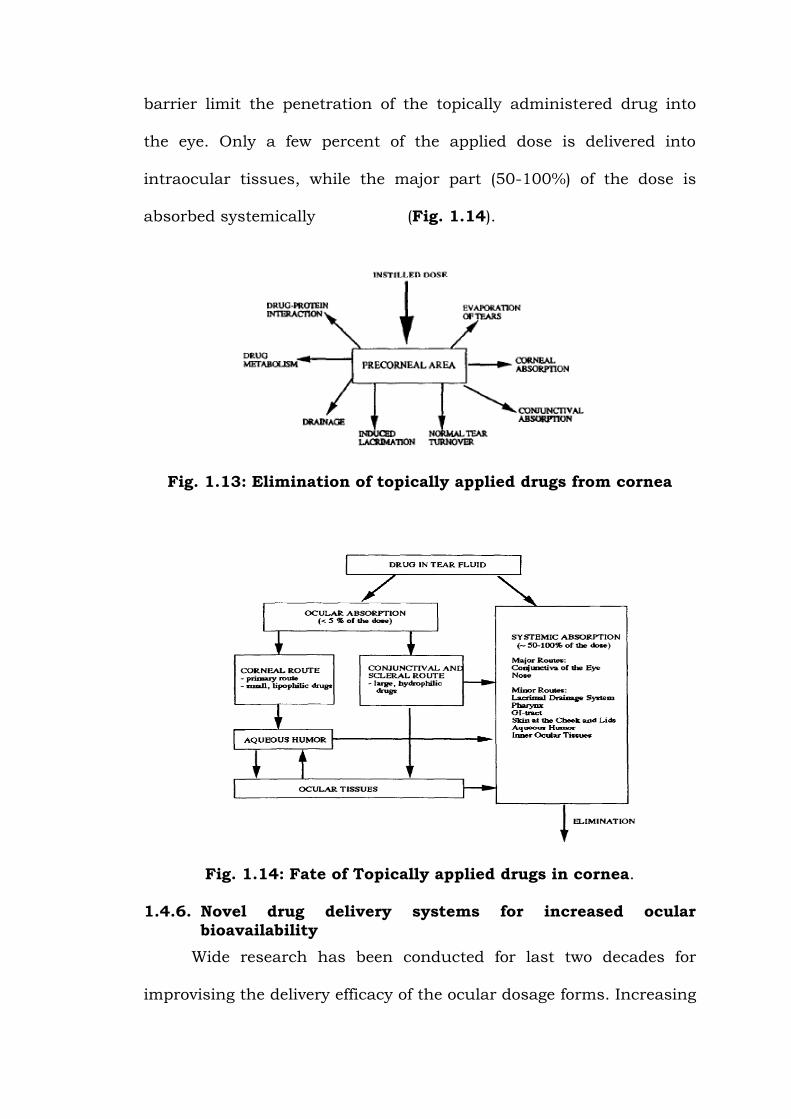
barrier limit the penetration of the topically administered drug into
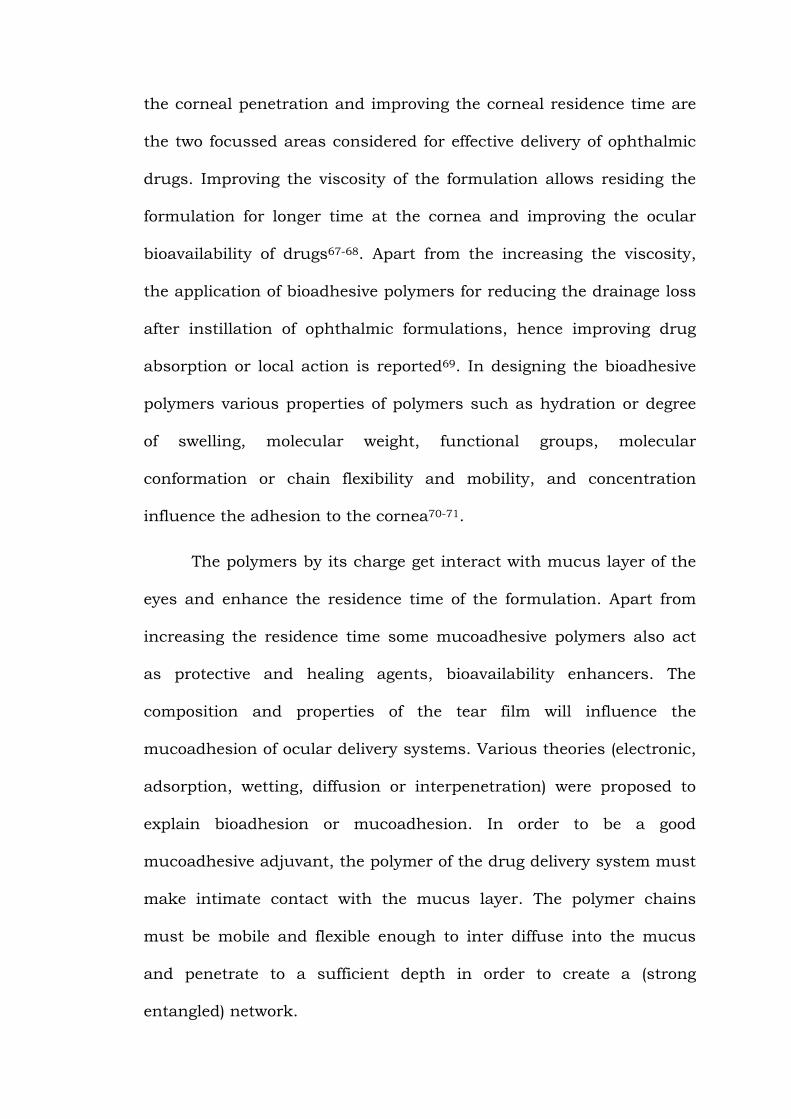
the eye. Only a few percent of the applied dose is delivered into
intraocular tissues, while the major part (50-100%) of the dose is
absorbed systemically (Fig. 1.14).
Fig. 1.13: Elimination of topically applied drugs from cornea
Fig. 1.14: Fate of Topically applied drugs in cornea.
1.4.6. Novel drug delivery systems for increased ocular
bioavailability
Wide research has been conducted for last two decades for
improvising the delivery efficacy of the ocular dosage forms. Increasing
the corneal penetration and improving the corneal residence time are
the two focussed areas considered for effective delivery of ophthalmic
drugs. Improving the viscosity of the formulation allows residing the
formulation for longer time at the cornea and improving the ocular
bioavailability of drugs67-68. Apart from the increasing the viscosity,
the application of bioadhesive polymers for reducing the drainage loss
after instillation of ophthalmic formulations, hence improving drug
absorption or local action is reported69. In designing the bioadhesive
polymers various properties of polymers such as hydration or degree
of swelling, molecular weight, functional groups, molecular
conformation or chain flexibility and mobility, and concentration
influence the adhesion to the cornea70-71.
The polymers by its charge get interact with mucus layer of the
eyes and enhance the residence time of the formulation. Apart from
increasing the residence time some mucoadhesive polymers also act
as protective and healing agents, bioavailability enhancers. The
composition and properties of the tear film will influence the
mucoadhesion of ocular delivery systems. Various theories (electronic,
adsorption, wetting, diffusion or interpenetration) were proposed to
explain bioadhesion or mucoadhesion. In order to be a good
mucoadhesive adjuvant, the polymer of the drug delivery system must
make intimate contact with the mucus layer. The polymer chains
must be mobile and flexible enough to inter diffuse into the mucus
and penetrate to a sufficient depth in order to create a (strong
entangled) network.
1.4.7. Thiomer preparations in ocular drug delivery
The so far described mucoadhesive polymers forms non covalent
bond with tear film and may not be sufficient enough to increase the
residence time of the formulation at the cornea. In the process of
exploiting the new polymers, thiomers have been designed. Thiomers
are thiol bearing polymers and helps in the formation of covalent
linkage with cornea. The rationale of the strategy is based on
knowledge concerning the role of disulfide bridges in the three-
dimensional mucin network formation72. Thiolated polymers, or so
called thiomers, are capable of forming covalent bonds with cysteine-
rich subdomains of mucins, where as mucoadhesive polymers
discussed so far formed non-covalent bonds (hydrogen bonds or ionic
interactions) with mucus, or exhibited physical entanglements73. The
schematic representation of interactions of thiomers with mucin
present on mucosa was given in Fig. 1.15. The extensive cross-linking
process of the thiomers with mucins resulted in a tremendous
increase in viscosity and mucoadhesion independent of pH or ionic
strength of the medium. The mucoadhesive properties of a chitosan
thioglycolic acid conjugate and a poly(acrylic acid)–cysteine conjugate
improved 10-fold and even 100-fold, respectively, compare to the
native polymers74-75. The thiomer formulation improve the cohesive
properties by a simple oxidation process in aqueous media and results
in the formation of inter- and/or intrachain disulfide bonds within the
polymeric network76. And also some of the thiomers have permeation
capability and promote the paracellular uptake of drugs by opening
the tight junctions. An in vitro study on the cornea of rabbits with
polycarbophil–cysteine showed a 2.2-fold and 2.4-fold increase in the
transcorneal permeation of sodium fluorescein and dexamethasone
phosphate, respectively, when compared to the unmodified poly
carbophil. Thiomers could be useful additives in artificial tear
formulation due to anti oxidative and radical scavenging properties.
Moreover, thiomers are similar to ocular mucins displaying numerous
thiol groups. Thiomers also mimic the physiological process of the
mucus layer such as tear film stabilization. The formation of disulfide
bonds with mucins leads to strong mucoadhesion, prolonged
residence time and protective effect for the corneal/conjunctival
epithelium. Considering mucoadhesion of thiomers based on covalent
bond formation with mucins, inserts (diameter 2mm) consisting of
PAA 450–cysteine conjugate, a thiolated poly(acrylic acid) 450 kDa,
were prepared by direct compression and evaluated by
fluorophotometry. In humans, the inserts based on thiolated
poly(acrylic acid) or PAA 450–cysteine conjugate provided a sufficient
fluorescein concentration in the tear film for more than 8 h. Inserts
made of thiomers were not soluble, and had good cohesive properties,
due to the formation of inter- and/or intra chain disulfide bonds
within the polymeric network after hydration. The general irritation
score indicated that the inserts were well accepted and tolerated77.
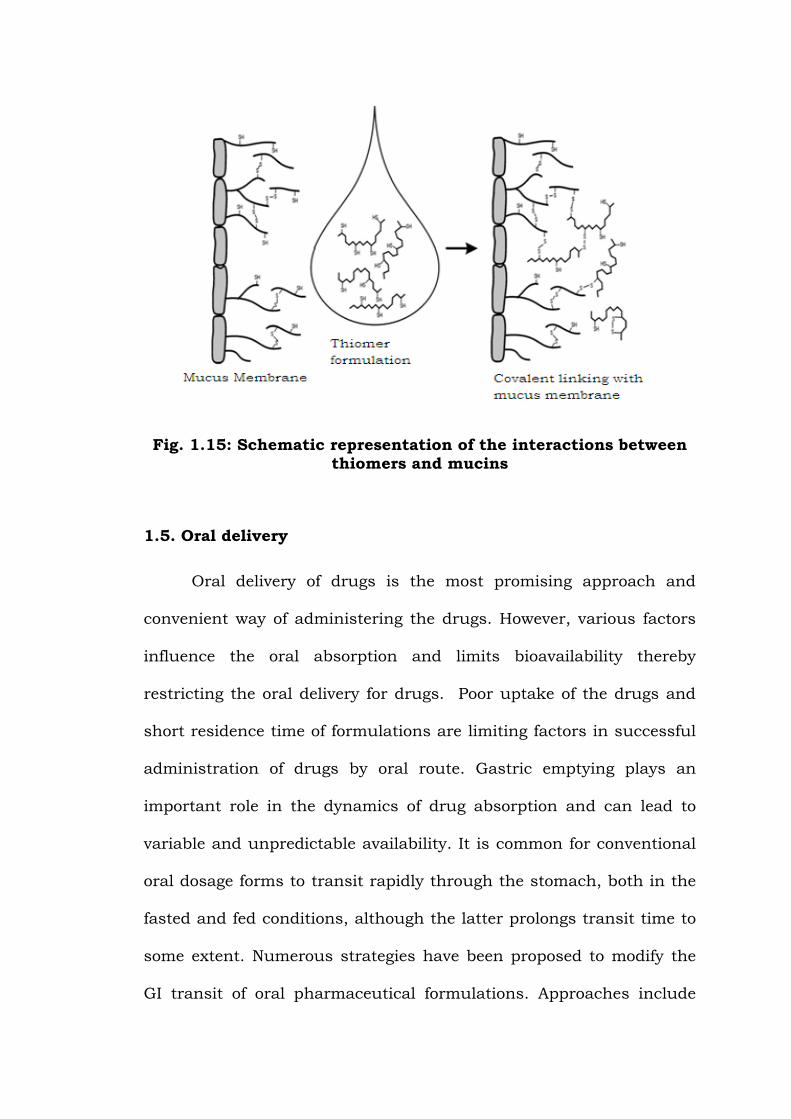
Fig. 1.15: Schematic representation of the interactions between thiomers and mucins
1.5. Oral delivery
Oral delivery of drugs is the most promising approach and
convenient way of administering the drugs. However, various factors
influence the oral absorption and limits bioavailability thereby
restricting the oral delivery for drugs. Poor uptake of the drugs and
short residence time of formulations are limiting factors in successful
administration of drugs by oral route. Gastric emptying plays an
important role in the dynamics of drug absorption and can lead to
variable and unpredictable availability. It is common for conventional
oral dosage forms to transit rapidly through the stomach, both in the
fasted and fed conditions, although the latter prolongs transit time to
some extent. Numerous strategies have been proposed to modify the
GI transit of oral pharmaceutical formulations. Approaches include
formulations that swell or expand in the gastric content and are
retained in the stomach by floating on the gastric contents or else are
too large to pass through the pylorus78-79. Alternative potential
approach is to design a mucoadhesive formulation which can adhere
to the lining of the stomach or small intestine, thus retaining the drug
at the target absorption site for a prolonged period.
1.5.1. Mucoadhesion approach for oral drug delivery
In order to develop an ideal oral bioadhesive system it is
important to have a thorough understanding of mucosa, bioadhesive
polymers and mucin-polymer interactions in the physiological
environment. Mucoadhesive drug delivery systems exploit the
attraction between polymers used in drug formulations and the
mucus layer that covers epithelial surfaces throughout the body,
including the gastrointestinal tract80-81. Mucus occurs in vivo both as
a gel layer that adheres strongly to mucosal surfaces and as a luminal
soluble or suspended forms82. Mucus gels consist more than 95% of
water and thoroughly hydrate the other mucus components: lipids,
inorganic salts, and mucins. Mucins tend to have a blocky
architecture: most of the glycans are confined to certain densely
glycosylated regions of the chain, separated from each other by
‗‗naked‘‘ protein stretches bearing only few sugar residues. Mucins are
large macromolecules, with molecular weights ranging from 10 to 50 ·
106 g/mol. They tend to assemble into even larger assemblies, via
hydrophobic interactions between amino acid residues, hydrogen
bonding among sugar units, or disulfide linkages involving cysteines83.
This variability among mucus throughout the body suggests roads
towards site-specific delivery of mucoadhesive drug formulations
through control, on the molecular level, of the interactions between
mucins and mucoadhesive polymers84.
Various investigators have proposed different mucin-polymer
interactions, such as:
Wetting and swelling of the polymer to permit intimate contact
with the biological tissue;
Interpenetration of bioadhesive polymer chains and
entanglement of polymer and mucin chains;
Formation of weak chemical bonds
Sufficient polymer mobility to allow spreading
Water transport followed by mucosal dehydration.
As the mucus layer comes into contact with bioadhesive coated
system, various non specific (van der walls, hydrogen bonding and /or
hydrophobic interactions) or specific interactions occur between the
complimentary structures. In order to improve the targeting and
delivery of orally administered drugs to the stomach and the small
intestine, the interest in mucoadhesive polymers has greatly increased
in the last two decades. The use of these polymers as carriers is
supposed to enhance the bioavailability of orally given drugs because
of a lengthened contact time of the drug with the gastrointestinal (GI)
mucosa. When mucoadhesive polymers also exhibiting permeation
enhancing properties are used, the intensified contact with the
mucosa should provide the prerequisite for an increased epithelial
permeability for many drugs mediated by the polymeric carrier
system.
1.5.2. Bioadhesive polymers
Bioadhesive polymers can be defined as natural or synthetic
materials capable of adhering to the biological substrate for an
extended duration. The extended duration should be sufficient time to
allow for a reduced frequency of administration compared to
conventional non bioadhesive polymers. The key attributes of
polymers contributing to bioadhesion are:
Sufficient quality of hydrogen bonding functional groups (-OH-
and –COOH)
High molecular weight and chain flexibility
Anionic surface charges
Adequate surface tension to promote spreading into the mucus
layer
Surface anchored groups with affinity to form bridges between
polymer and mucin.
1.5.3. Desired attributes of bioadhesive polymers for target oral delivery
In order for a bioadhesive polymer to work effectively, it should
possess the following multifunctional physio chemical properties
appropriate for oral drug delivery system:
Rapid adherence to mucosa
Demonstrate strong interactions with the mucin epithelial
tissue
Regenerate new bioadhesive surface and thus maintain
adherence over longer duration
Remain unaffected by the hydrodynamic conditions, food and
pH changes
Maintain bioadhesiveness upon hydration
Available in different bioadhesive grades for different
applications
Able to work effectively with various classes of BCS drugs
Minimum impact on the drug release
No breakdown at the mucosa
Wide margin of safety both locally and systemically
Easy to incorporate into various dosage forms
Long shelf life
Low cost.
1.5.4. Thiomers oral drug delivery
Because of advantages with the mucoadhesive systems,
numerous attempts have been undertaken in order to improve the
mucoadhesive properties of polymeric excipients. The mucoadhesive
properties of the first studied polymers were based on the formation of
non-covalent bonds such as hydrogen bonds and ionic interactions
with the mucus layer. The most commonly bridging structure in
biological systems, the disulfide bond, is thereby utilized to improve
adhesion of polymeric carrier systems to mucosal membranes. This
new generation of mucoadhesive polymers is based on so-called
thiomers. Thiomers are polymers bearing thiol groups that lead to the
formation of disulfide bonds with cysteine-rich subdomains of mucus
glycoproteins, the main constituents of the mucus layer covering
gastro-intestinal epithelia85. Thiolated polymers, are believed to
interact with cysteine-rich subdomains of mucus glycoproteins
forming disulfide bonds between the mucoadhesive polymer and the
mucus layer. Owing to the immobilization of thiol groups on already
well-established mucoadhesive polymers, their mucoadhesive
properties are strongly enhanced. Examples for this improved
mucoadhesion are given in Table1.1. Covalent bonds are believed to
be formed not only between thiomer and mucus, but also within the
thiomer itself. This theory was confirmed by the decrease in free thiol
groups within thiomers resulting in an increase in Viscosity86. Inter-
and intramolecular disulfide bonds improve the cohesive properties of
the thiolated polymer compared to the unmodified polymer. In
addition, the cohesive properties within the mucus gel layer are also
enhanced. Because disulfide bonds are formed during and after
thiomer mucus interpenetration, the mucus layer on which the
delivery system is adhering becomes comparatively more stable so
that the adhesive bond does not fail within the mucus gel layer itself.
Although thiomers show strongly increased mucoadhesive properties,
the adhesion of delivery systems being based on such polymers is
nevertheless limited by the natural mucus turnover. The mucus
turnover in the human intestine, for instance, was determined to be in
the range of 12–24 h87. Time of adhesion is therefore limited by this
permanent renewal process to several hours. These efficacies of
thiomers can be explained by the fact that the thiomers combines two
different mechanisms of mucoadhesion: (a) improved ionic
interactions between polymer and membrane and (b) the formation of
disulfide bonds due to the introduction of thiol. Huge literature is
available showing the potential of thiomers in enhancing the contact
time, bioavailability and permeation of administered small molecule
drugs, proteins and peptides88-90.
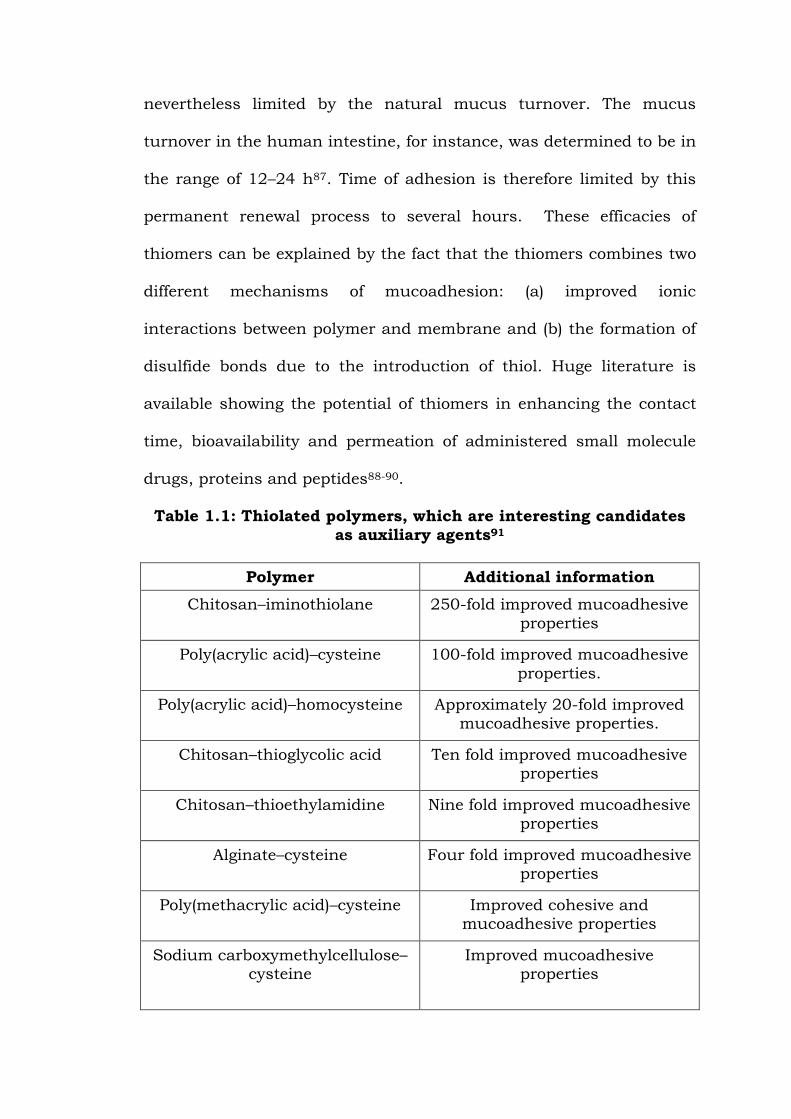
Table 1.1: Thiolated polymers, which are interesting candidates
as auxiliary agents91
Polymer Additional information
Chitosan–iminothiolane
250-fold improved mucoadhesive
properties
Poly(acrylic acid)–cysteine
100-fold improved mucoadhesive
properties.
Poly(acrylic acid)–homocysteine
Approximately 20-fold improved
mucoadhesive properties.
Chitosan–thioglycolic acid
Ten fold improved mucoadhesive properties
Chitosan–thioethylamidine
Nine fold improved mucoadhesive properties
Alginate–cysteine
Four fold improved mucoadhesive properties
Poly(methacrylic acid)–cysteine
Improved cohesive and mucoadhesive properties
Sodium carboxymethylcellulose–cysteine
Improved mucoadhesive properties
1.6. Nasal delivery
Nasal drug delivery has been recognized as potential route from
ancient days and nowadays it becomes an important tool in the
treatment of various disorders. Even though nasal route is practised
primarily for the treatment of local disorders, in the modern days it‘s
been exploited for the systemic application of many drugs including
protein and peptide molecules. For the last two decades numerous
articles and reviews have been published emphasizing the potential of
nasal drug delivery92-94. Nasal route, because of its richly supplied
vascular nature of nasal mucosa, has received a great deal of focus as
a convenient and reliable method for the systemic administration of
drugs, especially those which are ineffective orally and must be
administered by injection. The therapeutic agents which are
susceptible for hepatic metabolism or poor permeability in the GI tract
can be administered by nasal route for effective delivery of such drugs.
The ideal properties of drugs to be considered for nasal drug
delivery:
Used chronically
Ineffective orally
Used in small doses
Rapid entry to the general circulation is desirable
Rapid entry to CNS
1.6.1. Advantages of nasal drug delivery
Rapid absorption, higher bioavailability, therefore lower
doses
Avoidance of liver first pass metabolism
Fast onset of therapeutic action
Avoidance of metabolism by the gastrointestinal tract
Avoidance of irritation of the gastrointestinal membrane
Reduced risk of overdose
Non-invasive, therefore, reduced risk of infection
Ease of convenience and self-medication
Improved patient compliance
Can be a beneficial adjunct product to an existing
product;
Reduced risk of infectious disease transmission.
1.6.2. Limitations of nasal drug delivery
Not all are drugs are nasally permeable
Amount of administered volume is low (25-200 µl)
Some drugs may cause nasal irritation.
Some drugs may undergo metabolic degradation
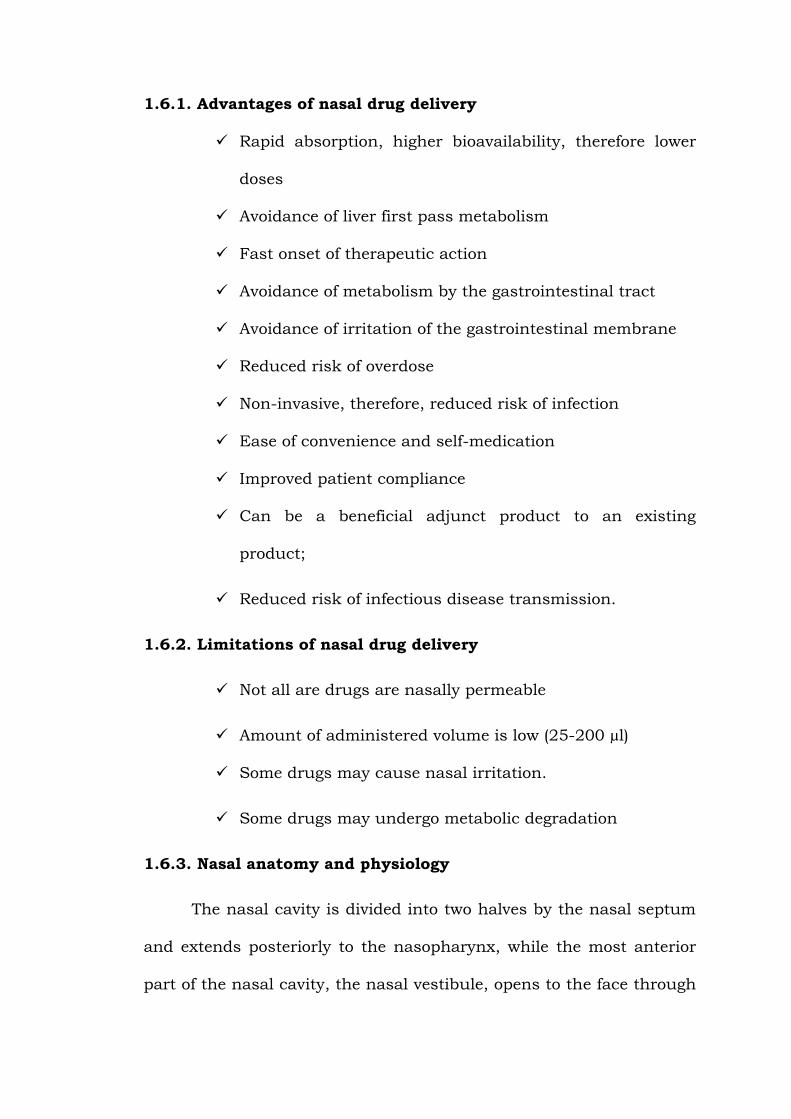
1.6.3. Nasal anatomy and physiology
The nasal cavity is divided into two halves by the nasal septum
and extends posteriorly to the nasopharynx, while the most anterior
part of the nasal cavity, the nasal vestibule, opens to the face through
the nostril (Fig. 1.16). The atrium is an intermediate region between
the vestibule and the respiratory region. The respiratory region, the
nasal conchae or turbinates, which occupies the major part of the
nasal cavity, possesses lateral walls dividing it into 3 sections: the
superior, middle and inferior nasal turbinates. These folds provide the
nasal cavity with a very high surface area compared to its small
volume. The epithelial cells in the nasal vestibule are stratified,
squamous and keratinized with sebaceous glands. Due to its nature,
the nasal vestibule is very resistant to dehydration and can withstand
noxious environmental substances and limits permeation of
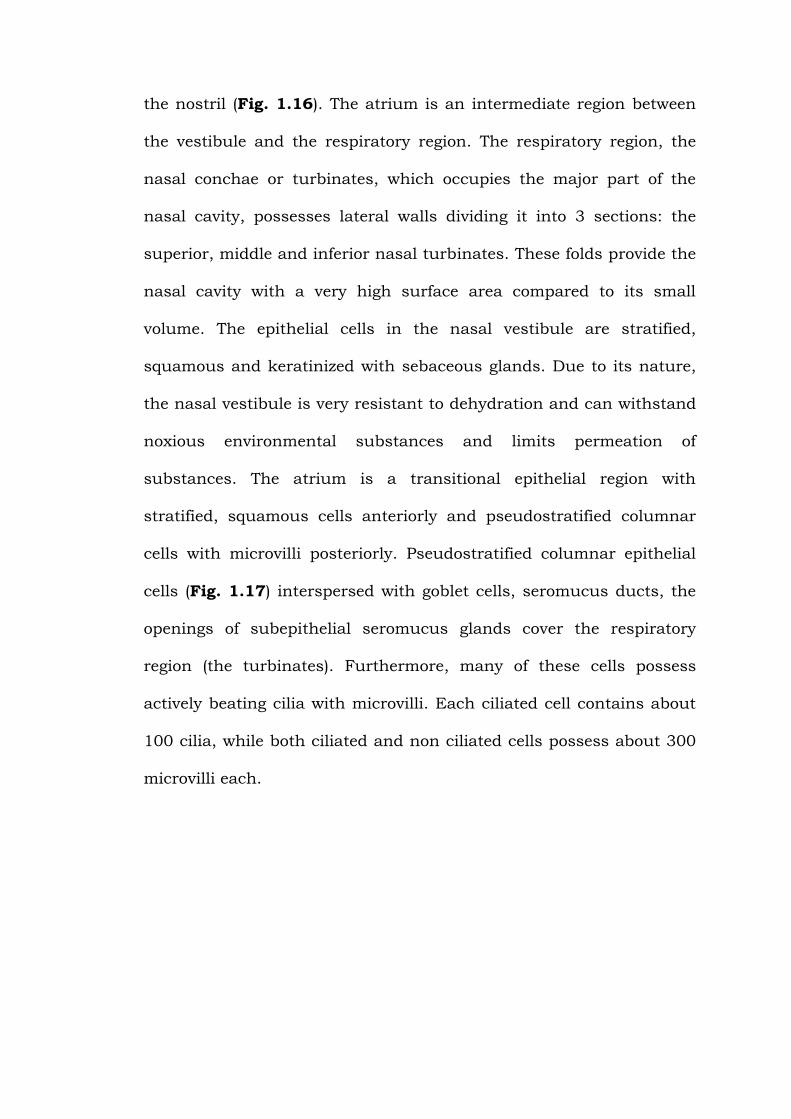
substances. The atrium is a transitional epithelial region with
stratified, squamous cells anteriorly and pseudostratified columnar
cells with microvilli posteriorly. Pseudostratified columnar epithelial
cells (Fig. 1.17) interspersed with goblet cells, seromucus ducts, the
openings of subepithelial seromucus glands cover the respiratory
region (the turbinates). Furthermore, many of these cells possess
actively beating cilia with microvilli. Each ciliated cell contains about
100 cilia, while both ciliated and non ciliated cells possess about 300
microvilli each.
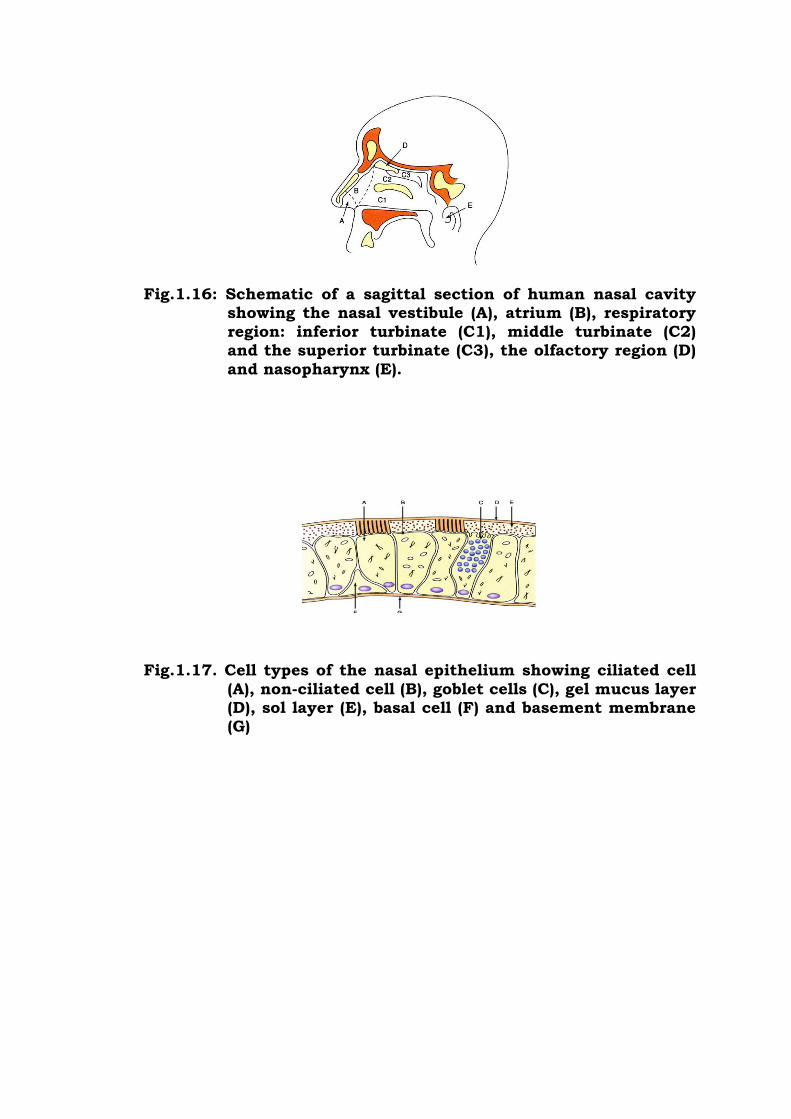
Fig.1.16: Schematic of a sagittal section of human nasal cavity showing the nasal vestibule (A), atrium (B), respiratory
region: inferior turbinate (C1), middle turbinate (C2) and the superior turbinate (C3), the olfactory region (D)
and nasopharynx (E).
Fig.1.17. Cell types of the nasal epithelium showing ciliated cell
(A), non-ciliated cell (B), goblet cells (C), gel mucus layer (D), sol layer (E), basal cell (F) and basement membrane (G)
Table 1.2: Structural features of different sections of nasal cavity and their relative impact on permeability95
Region Structural features Permeability
Nasal vestibule Nasal hairs(vibrissae)
Epithelial cells are stratified, squamous and keratinized
Sebaceous glands present
Least permeable because of the presence of keratinized cells
Atrium Transcpicthelial region
Stratified squamous
cells present interiorly and pseudo stratified cells with microvilli present posteriorly
Less permeable as it has small surface area
and stratified cells are present anteriorly
Respiratory region (inferior turbinate middle turbinate superior turbinate)
Pseudo stratified columnar cells with microvilli (300 per cell), large surface area
Receives maximum nasal secretions because of the presence of seromucus glands, nasolacrimal duct and goblet cells
Richly supplied with blood for heating and humidification of inspired air, presence of paranasal sinuses
Most permeable region because of large surface area and rich vasculature
Olfactory region Specialized ciliated olfactory nerve cells for smell perception
Receives ophthalmic and maxillary divisions of trigeminal nerve
Direct access to cerebrospinal fluid
Direct access to cerebrospinal fluid
Nasopharynx Upper part contains ciliated cells and lower part contains squamous epithelium
Receives nasal cavity drainage
With the initial success in the development of nasal delivery
products has led to intensive research, however the enthusiasm was
confronted with disappointing in vivo results showing poor
bioavailability. The reasons for the failure seem to be the low
residence time of the formulations in the nasal tract. Apart from this
low permeability and enzymatic degradation also considered as the
culprits for the failure. This failure led to the development of new
strategies, consequently the use of mucoadhesive polymers based
formulations demonstrated enhanced residence time and permeation
enhancing capabilities96-97. The encouraging results and the desire to
overcome some new challenges stimulated the development of new
generations of polymers based on pH or thermal responsiveness or
modified existing polymers having improved bioadhesive or
permeation-enhancing properties98-99.
1.6.4. The factors that influence nasal drug delivery (NDD) as
potential route
A large surface area available for drug deposition and
absorption. The effective absorptive surface area of the nasal
epithelium is even higher as a result of the presence of
microvilli.
The nasal epithelium is thin, porous (especially when compared
to other epithelial surfaces) and highly vascularized. This
ensures high degree of absorption and rapid transport of
absorbed substances into the systemic circulation for initiation
of therapeutic action.
A porous endothelial basement membrane that poses no
restriction to transporting the drug into general circulation.
Absorbed substances are transported directly into the systemic
circulation thereby avoiding the first pass metabolic effect
generally experienced following oral drug administration.
In some cases, drugs can be absorbed directly into the CNS
after nasal administration bypassing the tight blood–brain
barrier.
Generally speaking, the enzymatic activity of the nasal
epithelium is lower than that of the GIT or liver and higher
bioavailability of drugs especially proteins and peptides can be
achieved. In addition, enzyme inhibitors are more effective
following nasal than oral application because of a higher degree
of dilution in the latter than in the former.
Realization of pulsatile delivery of some drugs like human
growth hormone, insulin, etc., is higher with NDD.
The nose is amenable to self-medication that not only lowers the
cost of therapy but improves patient compliance as well. The
risk of over-dosage is low and nasal lavage can be used to
remove unabsorbed excess drug.
Reformulation of existing drugs as NDD products offers
companies the possibility to extend the life cycle of their
products
1.6.5. Mucoadhesion as a strategy to improve systemic drug delivery via the nasal route
As an alternative to the oral and parenteral route of
administration, nasal route has emerged as effective way for the
administration of small and large therapeutic moieties. A number of
approaches are used to counter the various limitations of nasal drug
administration. The three major approaches that have been attempted
are: the use of chemical enhancers to improve absorption;
incorporation of enzyme inhibitors; and increasing drug local
residence time using mucoadhesive polymers. An alternative approach
to the use of chemical enhancers to improve nasal drug absorption is
to increase the duration of formulation residence within the nasal
cavity. This is achieved by the use of bioadhesive polymers.
1.6.6. New generation polymers used on nasal drug delivery
Initial research on nasal mucoadhesion employed polymers
manufactured for other purposes in the pharmaceutical and food
industries several different types of polymers have been employed for
delivery of different types/classes of drugs. In a lot of other cases only
marginal or even no successes were obtained. Further examination of
the causes of failure pointed lack of 1) tissue specificity with respect to
adhesion, (2) reduced adhesion time, (3) lack of permeation
enhancement capability, (4) interaction between drug and polymer
leading to decreased release of the drug from the dosage form,
increased drug instability, etc., and (5) toxicity induced by the
polymer. Efforts to overcome such problems have lead researchers to
develop new polymers, the so-called second-generation
mucoadhesives, a lot of which have been developed and tested for
nasal drug delivery. Even though the mechanism of adhesion is the
same at nasal or gastrointestinal tract sites, the fictionalization of the
polymers leads to more tissue/organ specificity to issues like (1)
delivery from devices and deposition in the appropriate region of the
nasal cavity, (2) lack of tissue specificity with respect to adhesion, (3)
reduced adhesion time, (4) lack of permeation enhancement
capability, (5) interaction between drug and polymer leading to
decreased release of the drug from the dosage form, increased drug
instability, etc., and (6) toxicity induced by the polymer.
1.6.7. Thiomers in nasal drug delivery
Pharmaceutical technological attempts to overcome these
barriers include the use of enzyme inhibitors, permeation enhancers
and multifunctional polymers ideally guaranteeing both enzyme
inhibition permeation enhancement and mucoadhesion. Among this
group of multifunctional polymers exhibiting all these mentioned
properties, thiolated polymers-designated thiomers—are the most
promising for nasal delivery. Due to the immobilisation of thiol groups
on well-established multifunctional polymers their enzyme inhibitory,
permeation enhancing and mucoadhesive properties can be strongly
improved. Recently, the potential of a thiomer gel formulation could be
demonstrated by in vivo studies. Leitner et al100 developed a nasal gel
formulation for systemic delivery of hGH. The efficacy of a
mucoadhesive gel formulation being based on unmodified
polycarbophil and polycarbophil–cysteine was compared in rats.
Results demonstrated a significantly higher and prolonged nasal
bioavailability of hGH, which was incorporated in the thiomer gel
formulation. Utilizing the thiomer gel formulation an absolute nasal
bioavailability of 2.75±0.37% was achieved. As thiomers also exhibit a
strong permeation enhancing effect, however, it is difficult to attribute
this improved in vivo efficacy exclusively to the improved
mucoadhesive properties. In another study thiolated polyacrylate
microparticles were generated for the nasal delivery of hGH. The
intranasal administration of this microparticulate formulation to rats
resulted in a relative bioavailability of 8.11±2.15% that represents a 3-
fold improvement compared to microparticles comprising the
corresponding unmodified polymer.
1.6.8. Nose to brain delivery of drugs to the brain via the nasal
route
Recent research on the nasal delivery has highlighted the
possibility of exploiting this route for direct transport of drugs from
nose to brain. Absorption of drugs at the olfactory region of the nose
provides a potential for a therapeutic agent available in the brain.
Numerous studies in the animals provide the evidence for the
presence of a direct pathway from the olfactory region to the brain101-
103. Hence, nasally administered drugs might be able to reach a target
in the brain to a greater concentration that any other route. Reports in
the literature of studies in animal models and in man have shown this
to be a distinct possibility with results showing the uptake of drugs
into the cere-brospinal fluid and the brain tissue being dependent
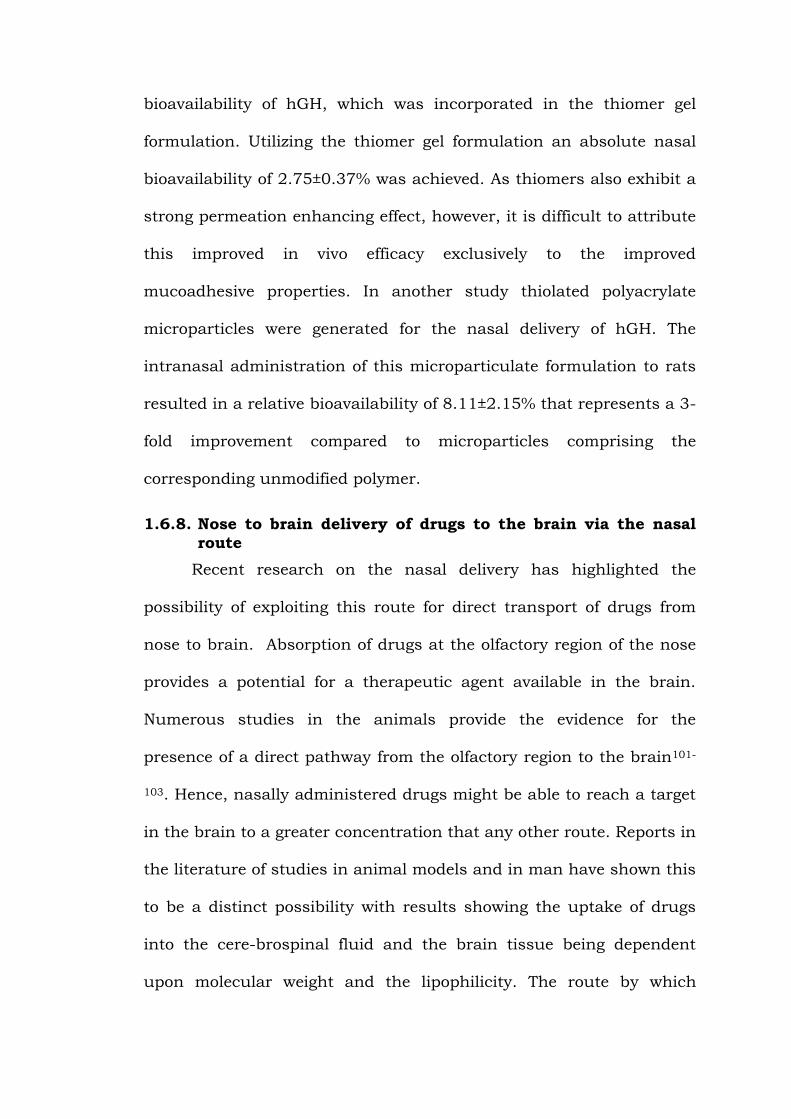
upon molecular weight and the lipophilicity. The route by which
nasally delivered drugs can reach the cerebro-spinal fluid (CSF),
which surrounds the brain and the actual brain tissue, is depicted in
the Fig.1.18. The drug can also follow the systemic pathway to reach
the brain by crossing the blood brain barrier but the use of this
pathway is highly dependent on the properties of the drug104. Of
special interest is the transport of drug across the olfactory region in
the nasal cavity directly into the brain tissue (e.g. olfactory bulb) or
the CSF. The olfactory epithelium is situated between the nasal
septum and the lateral wall of each side of the two nasal cavities and
just below the cribriform plate of the ethmoid bone separating the
nasal cavity from the cranial cavity. The drug can cross the olfactory
pathway by one or a combination of pathways105. Firstly, the drug can
use a transcellular pathway, where the drug is transferred by receptor
pathway, where the drug is transferred by receptor passive diffusion.
This pathway is especially suited for small lipophilic molecules or
large molecules. Secondly, the drug can use the para cellular pathway
by passing through the tight junctions or through open clefts in the
membrane. This pathway is especially suited for smaller hydrophilic
molecules. Thirdly, the drug can be transported through the olfactory
neuron cells by intracellular axonal transport primarily to the
olfactory bulb.
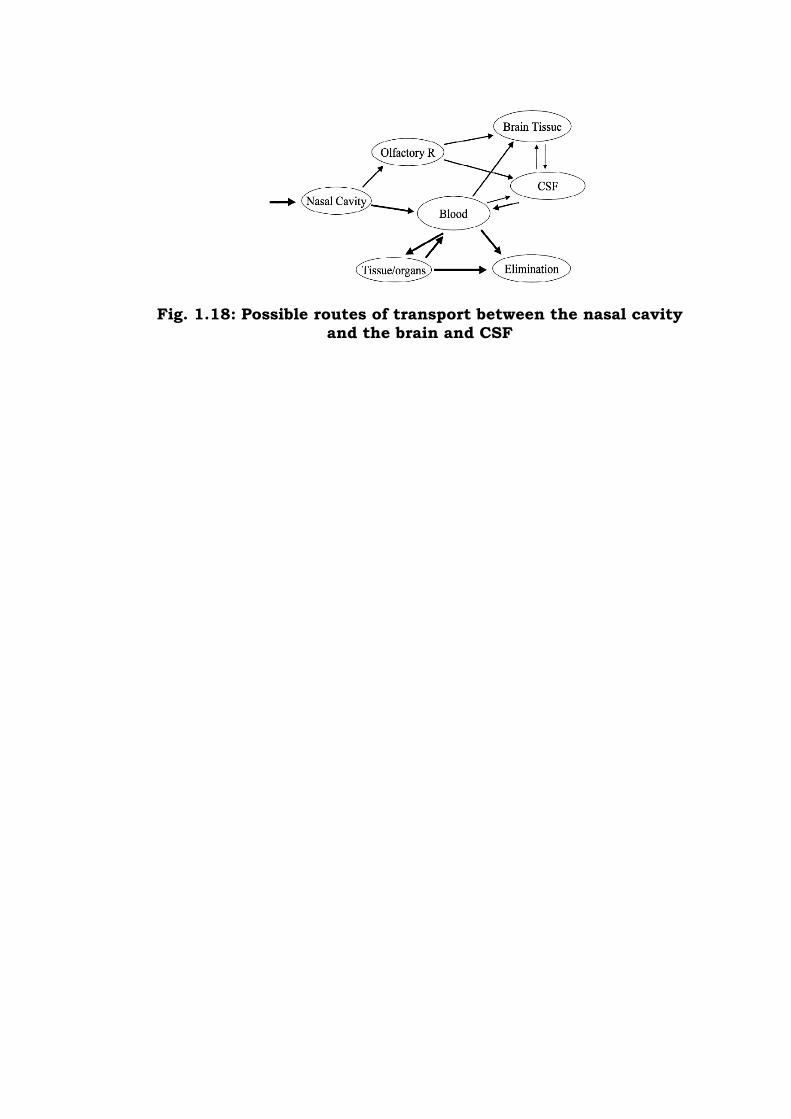
Fig. 1.18: Possible routes of transport between the nasal cavity and the brain and CSF
REFERENCES
1. J.M. Gu, J.R. Robinson, S.H.S. Leung, Binding of acrylic polymers
to mucin/epithelial surfaces: structure property relationships, Crit. Rev. Ther. Drug Carr. Syst., 5, 21–67, 1988.
2. N.A. Peppas, J.J. Sahlin, Hydrogels as mucoadhesive and bioadhesive materials: a review, Biomaterials, 17, 1553– 1561, 1996.
3. C. Marriott, N.P. Gregory, Mucus physiology and pathology, in: V. Lanaerts, R. Gurny (Eds.), Bioadhesive Drug Delivery Systems, CRC Press, Florida, 1 – 24, 1990.
4. W.J, Allen, J.P. Cunliffe, C.W. Pearson, Venables, The adherent gastric mucus gel barrier in man and changes in peptic
ulceration, J. Intern. Med., 228, 83–90, 1990.
5. S. Kerss, A. Allen, A. Garner, A simple method for measuring the thickness of the mucus gel layer adherent to rat, frog, and human
gastric mucosa: influence of feeding, prostaglandin, Nacetylcysteine and other agents, Clin. Sci., 63, 187–195, 1982.
6. T. Sonju, T.B. Cristensen, L. Kornstad, G. Rolla, Electron microscopy, carbohydrate analysis and biological activities of the proteins adsorbed in two hours to tooth surfaces in vivo,
Caries. Res., 8, 113– 122, 1974.
7. R.P. Ahuja, R.P. Khar, J. Ali, Mucoadhesive drug delivery systems,
Drug Dev. Ind. Pharm., 23, 489– 515, 1997.
8. E. Mathiowitz, D.E. Chickering, Definitions, mechanisms and theories of bioadhesion, in: E. Mathiowitz, D.E. Chickering,C.-M.
Lehr (Eds.), Bioadhesive Drug Delivery Systems: Fundamentals, Novel Approaches and Development, Marcel Decker, New York, 1 –10, 1999.
9. A.T.Florence, D. Attwood, Physicochemical Principles of
Pharmacy, Third edition, Palgrave Ltd, Basingstoke, 76-86, 1997.
10. S.A. Mortazavi, J.D. Smart, An investigation of some factors influencing the in-vitro assessment of mucoadhesion,
Int. J.Pharm., 116, 223– 230, 1995.
12. D. Smart, I.W. Kellaway, H.E.C. Worthington, An in vitro investigation of mucosa-adhesive materials for use in controlled
drug delivery, J. Pharm. Pharmacol., 36, 295– 299, 1984.
13. J.D. Smart, Drug delivery using buccal adhesive systems, Adv.
Drug Deliv. Rev., 11, 253–270, 1993.
14. O. Ben Zion, A. Nussinovitch, Physical properties of hydrocolloid wet glues, Food Hydrocoll., 11, 429– 442, 1997.
15. A. Bernkop-Schnurch, S. Scholler, R.G. Biebel, Development of controlled release systems based on thiolated polymers, J.
Control. Rel., 66, 39–48, 2000.
16. A. Bernkop-Schnurch, C.E. Kast, M.F. Richter, Improvement in the mucoadhesive properties of alginate by the covalent
attachment of cysteine, J. Control. Rel., 71, 277–285, 2001.
17. A.H. Shojaei, J. Paulson, S. Honary, Evaluation of poly(acrylic acid-co-ethylhexyl acrylate) films for mucoadhesive transbuccal
drug delivery: factors affecting the force of mucoadhesion, J. Control. Rel., 67, 223–232, 2000.
18. Y. Huang, W. Leobandung, A. Foss, N.A. Peppas, Molecular aspects of muco- and bioadhesion: tethered structures and site specific surfaces, J. Control. Rel., 65, 63– 71, 2001.
19. P. Bures, Y. Huang, E. Oral, N.A. Peppas, Surface modifications and molecular imprinting of polymers in medical and
pharmaceutical applications, J. Control. Rel., 72, 25– 33, 2001.
20. B.S. Lelle, A.S. Hoffman, Mucoadhesive drug carriers based on complexes of polyacrylic acid and PEGylated drugs having
hydrolysable PEG-anhydride-drug linkages, J. Control. Rel., 69, 237– 248, 2000.
21. L.E. Bromberg, Enhanced nasal retention of hydrophobically
modified polyelectrolytes, J. Pharm. Pharmacol., 53, 109– 114, 2001.
22. K. Huang, B.P. Lee, D.R. Ingram, P.M. Messersmith, Synthesis and characterization of self assembling block copolymers containing bio adhesive end groups, Biomacromolecules., 3,
397–406, 2002.
23. C.-M. Lehr, Lectin-mediated drug delivery: the second generation of bioadhesives, J. Control. Rel., 65, 19– 29, 2000.
24. A.Bernkop-Schnurcha,, A.H. Krauland, M.V. Leitnerb, T. Palmberger, Thiomers: potential excipients for non-invasive
peptide delivery systems, Eur. J. Pharm. Biopharm., 58, 253–263, 2004.
25. A. Bernkop-Schnurch, V. Schwarz, S. Steininger, Polymers with
thiol groups: a new generation of mucoadhesive polymers? Pharm. Res., 16, 876–881, 1999.
26. A. Bernkop-Schnurch, M. Hornof, T. Zoidl, Thiolated polymers—thiomers: modification of chitosan with 2-iminothiolane,
Int. J. Pharm., 260, 229–237, 2003.
27. V.M. Leitner, G.F. Walker, A. Bernkop-Schnurch, Thiolated
polymers: evidence for the formation of disulphide bonds with mucus glycoproteins, Eur. J. Pharm. Biopharm., 56, 207–214, 2003.
28. M.K. Marschutz, A. Bernkop-Schnurch, Thiolated polymers: self cross linking properties of thiolated 450 kDa poly(acrylic acid) and their influence on mucoadhesion, Eur. J. Pharm. Sci., 15, 387–
394, 2002.
29. A. Bernkop-Schnurch, V. Konig, V. Leitner, A. Krauland, I.
Brodnik, Preparation and characterization of thiolated poly(methacrylic acid)-starch compositions, Eur. J. Pharm. Biopharm., 57, 219–224,2004.
30. D. Guggi, M.K. Marschutz, A. Bernkop-Schnurch, Matrix tablets based on thiolated poly(acrylic acid): pH-dependent variation in
disintegration and mucoadhesion, Int. J. Pharm., 274,97–105, 2004.
31. A. Bernkop-Schnurch, S.C. Thaler, Polycarbophil–cysteine
conjugates as platforms for oral polypeptide delivery systems, J. Pharm.Sci., 89, 901–909, 2000.
32. A.E. Clausen, A. Bernkop-Schnurch, In vitro evaluation of the
permeation-enhancing effect of thiolated polycarbophil, J. Pharm. Sci., 89, 1253–1261, 2000.
33. C.E. Kast, A. Bernkop-Schnurch, Influence of the molecular mass on the permeation enhancing effect of different poly(acrylates), STP Pharma Sci., 12, 351–356, 2002.
34. A.E. Clausen, A. Bernkop-Schnu¨rch, In vitro evaluation of matrix tablets based on thiolated polycarbophil, Pharm. Ind. 63,
312–317, 2001.
35. A. Bernkop-Schnurch, M.D. Hornof, C.E. Kast, N. Langoth, Thiolated polymers: stability of thiol moieties under different
storage conditions, Sci. Pharm. 70, 331–339, 2002.
36. E. Buhleier, W. Wehner, F. Vögtle, "Cascade"- and "nonskid-
chain-like" syntheses of molecular cavity topologies. Synthesis (Mass.), 155–158, 1978.
37. R.G.Denkewalter, J. Kolc, W.J.Lukasavage, Macromolecular
highly branched homogeneous compound based on lysine units.
US Patent 4,289,872, 1981.
38. D.A. Tomalia, A new class of polymers-starburst-dendritic
macromolecules. Polym. J., 17, 117–132, 1985.
39. G.R.Newkome, Z. Yao, G.R. Baker, V.K. Gupta, Micelles. Part 1.
Cascade molecules: a new approach to micelles. A [27]-arborol. J. Org. Chem., 50, 2003–2004, 1985.
40. J.M.J. Fréchet, D.A. Tomalia, Dendrimers and Other Dendritic
Polymers. John Wiley & Sons, Chichester, New York, USA, 2001.
41. D.A.Tomalia, A.M. Naylor, W.A. Goddard, Starburst dendrimers: molecular-level control of size, shape, surface chemistry, topology,
and flexibility from atoms to macroscopic matter. Angew. Chem. Int. Edn. Engl., 29, 138–175, 1990.
42. Y. Li, Controlled assembly of dendrimer-like DNA. Nat. Mater., 3, 38–42, 2004.
43. S.André, B. Liu, H.J. Gabius, R. Roy, First demonstration of
differential inhibition of lectin binding by synthetic tri- and tetravalent glycoclusters from cross-coupling of rigidified 2-
propynyl lactoside. Org. Biomol. Chem., 1, 3909–3916, 2003.
44. Y.H.Jiang, SPL7013 gel as a topical microbicide for prevention of vaginal transmission of SHIV89.6P in macaques. AIDS Res. Hum.
Retroviruses., 21, 207–213, 2005.
45. N.Malik, E.G. Evagorou, R.Duncan, Dendrimer-platinate: a novel approach to cancer chemotherapy. Anticancer Drugs, 10,
767–776, 1999.
46. J.F.Kukowska-Latallo, Nanoparticle targeting of anticancer drug
improves therapeutic response in animal model of human epithelial cancer. Cancer Res., 65, 5317–5324, 2005.
47. E.C.Wiener, Dendrimer-based metal chelates: a new class of
magnetic resonance imaging contrast agents. Magn. Reson. Med. 31, 1–8, 1994.
48. I.Dunphy, S.A.Vinogradov, D.F. Wilson, Oxyphor R2 and G2:
phosphors for measuring oxygen by oxygen-dependent quenching of phosphorescence. Anal. Biochem., 310, 191–198, 2002.
49. S. Supattapone, H.O.B. Nguyen, F.E. Cohen, S.B. Prusiner, M.R.Scott, Elimination of prions by branched polyamines and implications for therapeutics. Proc. Natl. Acad. Sci. USA, 96,
14529–14534, 1999.
50. N.Bourne, Dendrimers, a new class of candidate topical
microbicides with activity against herpes simplex virus infection. Antimicrob. Agents Chemother., 44, 2471–2474, 2000.
51. J.Drobnik, F. Rypacek, Soluble synthetic polymers in biological systems. Adv. Polym. Sci., 57, 1–50, 1984.
52. N. Malik, Dendrimers: relationship between structure and biocompatibility in vitro and preliminary studies on the biodistribution of 125I-labelled polyamidoamine dendrimers in vivo.
J. Control. Rel., 65, 133–148, 2000.
53. R. Jevprasesphant, The influence of surface modification on the
cytotoxicity of PAMAM dendrimers. Int. J. Pharm. 252, 263–266, 2003.
54. H.T.Chen, M.F, Neerman, A.R. Parrish,E.E. Simanek, Cytotoxicity,
hemolysis, and acute in vivo toxicity of dendrimers based on melamine, candidate vehicles for drug delivery. J. Am. Chem.
Soc., 126, 10044–10048, 2004.
55. S.Watanabe, M.Sato, S Sakamoto, K. Yamaguchi, M. Iwamura, New dendritic caged compounds: synthesis, mass spectrometric
characterization, and photochemical properties of dendrimers with á-carboxy-2-nitrobenzyl caged compounds at their periphery.
J. Am. Chem. Soc. 122, 12588–12589, 2000.
56. M.Nishikawa, Y.Takakura, M.Hashida, Pharmacokinetic evaluation of polymeric carriers. Adv. Drug Deliv. Rev., 21,
135–155, 1996.
57. D.M. Maurice, S. Mishima, Ocular pharmacokinetics, in: M.L. Sears (Ed.), Handbook of experimental pharmacology, vol. 69,
Springer Verlag, Berlin-Heidelberg, pp. 16–119. 1984.
58. V.H.L. Lee, J.R. Robinson, Review: topical ocular drug delivery:
recent developments and future challenges. Ocul. Pharmacol., 2, 67–108, 1986.
59. L. Salminen, Review: systemic absorption of topically applied
ocular drugs in humans, J. Ocul. Pharmacol., 6, 243– 249, 1990.
60. C. Baudouin, Side effects of antiglaucomatous drugs on the
ocular surface, Curr. Opin. Ophthalmol., 7, 80–86, 1996.
61. J.C. Robinson, Ocular anatomy and physiology relevant to ocular drug delivery, in: A.K. Mitra (Ed.), Ophthalmic Drug Delivery
Systems, Marcel Dekker, New York, pp. 29– 57, 1993.
62. M. Van Ooteghem, Factors influencing the retention of ophthalmic solutions on the eye surface, in: M.F. Saettone, M. Bucci, P.
Speiser (Eds.), Ophthalmic Drug Delivery. Biopharmaceutical,
Technological and Clinical Aspects, Fidia Research Series, vol. 11, Livinia Press, Padova, 7 –17, 1987.
63. A. Urtti, L. Salminen, Minimizing systemic absorption of topically administered ophthalmic drugs, Surv. Ophthalmol., 37, 435–457,
1993.
64. A.Urtti, H. Rouhiainen, T. Kaila, V. Saano, Controlled ocular timolol delivery: systemic absorption and intraocular pressure
effects in humans, Pharm. Res., 11, 1278–1282, 1994.
65. M. Hornof, E. Toropainen, A. Urtti, Cell culture models of the ocular barriers, Eur. J. Pharm. Biopharm., 60, 207–225, 2005.
66. V.H.L Lee, J.R.Robinson, Mechanistic and quantitative evaluation of precorneal pilocarpine disposition in albino rabbits. J. Pharm.
Sci., 68, 673-684, 1979.
67. J.H. Trueblood, R.M. Rossomondo, W.H. Carlton, L.A.Wilson, Corneal contact times of ophthalmic vehicles. Evaluation by
microscintigraphy, Arch. Ophthalmol., 93, 127–130, 1975.
68. S.S. Chrai, J.R. Robinson, Ocular evaluation of methylcellulose
vehicle in albino rabbits, J. Pharm. Sci., 63, 1218– 1223, 1974.
69. J.W. Lee, J.H. Park, J.R. Robinson, Bioadhesive-based dosage forms: the next generation, J. Pharm. Sci., 89, 850–866, 2000.
70. M.F. Saettone, S. Burgalassi, P. Chetoni, Ocular bioadhesive drug delivery systems, in: E. Mathiowitz, D.E. Chickering, C.-M. Lehr (Eds.), Bioadhesive Drug Delivery Systems. Fundamentals, Novel
Approaches and Development, Marcel Dekker, Inc., New York, pp. 601– 640, 1999.
71. S.C. Chang, D.S. Chien, H. Bundgaard, V.H.L. Lee, Relative effectiveness of prodrug and viscous approaches in maximizing the ratio of ocular to systemic absorption of topically applied
timolol, Exp. Eye Res., 46, 56– 69, 1988.
72. K. Khanvilkar, M.D. Donovan, D.R. Flanagan, Drug transfer through mucus, Adv. Drug Deliv. Rev., 48, 173–193, 2001.
73. V.M. Leitner, G.F. Walker, A. Bernkop-Schnuerch, Thiolated polymers: evidence for the formation of disulphide bonds with
mucus glycoproteins, Eur. J. Pharm. Biopharm., 56, 207–214, 2003.
74. A. Bernkop-Schnuerch, Mucoadhesive polymers, use thereof and
method for producing the same. Patent EP 1126881, 1998.
75. C.E. Kast, A. Bernkop-Schnuerch, Thiolated polymers–thiomers:
development and in vitro evaluation of chito- san–thioglycoloc acid conjugates, Biomaterials, 22, 2345– 2352, 2001.
76. A. Bernkop-Schnuerch, S. Scholler, R.G. Biebel, Development of controlled release systems based on thiolated polymers,
J. Control. Rel., 66, 39–48, 2000.
77. M. Hornhof, W. Weyenberg, A. Ludwig, A. Bernkop-Schnuerch, Mucoadhesive ocular insert based on thiolated poly(acrylic acid):
development and in vivo evaluation in humans, J. Control. Rel., 89, 419– 428, 2003.
78. L.Khosla. The effect of polycarbophil on the gastric emptying of pellets. J. Pharm. Pharmacol. 39, 47–53, 1987.
79. D.Harris, GI transit of potential bioadhesive formulations in man:
A scintigraphic study. J. Control. Rel., 12, 45–49, 1990.
80. N.A. Peppas, A.G. Mikos, Kinetics of mucus-polymer interactions,
in:R. Gurny, H.E. Junginger (Eds.), Bioadhesion— Possibilities Future Trends, Wissenschaftliche Verlagsgesellschaft, Stuttgart, 65–85, 1990.
81. J.Jinno, D.M. Oh, J.R. Crison, G.L. Amidon, Dissolution of ionizable water-insoluble drugs: the combined effect of pH and surfactant, J. Pharm. Sci., 89, 268–274, 2000.
82. J.D. Smart, The basics and underlying mechanisms of mucoadhesion, Adv. Drug Deliv. Rev., 57, 1556–1568, 2005.
83. M.M. Patel, J.D. Smart, T.G. Nevell, R.J. Ewen, P.J. Eaton, J.Tsibouklis, Mucin/poly(acrylic acid) interactions: a spectroscopic investigation of mucoadhesion, Biomacromolecules,
4, 1184–1190, 2003.
84. L. Serra, J. Dome´nech, N.A. Peppas, Design of poly(ethylene
glycol)- tethered copolymers as novel mucoadhesive drug delivery systems,Eur. J. Pharm. Biopharm., 63, 11–18, 2006.
85. V.M. Leitner, A.Bernkop-Schnurch, Thiolated polymers: evidence
for the formation of disulphide bondswith mucus glycoproteins. Eur. J. Pharm. Biopharm., 56, 207–214, 2003.
86. A.Bernkop-Schnurch, Thiolated polymers – thiomers: synthesis
and in vitro evaluation of chitosan–2-iminothiolane conjugates. Int. J. Pharm., 260, 229–237, 2003.
87. C.E. Kast, A.Bernkop-Schnurch, Development and in vivo evaluation of an oral delivery system for low molecular weight
heparin based on thiolated polycarbophil. Pharm. Res. 20,
931–936, 2003.
88. P.Caliceti, A.Bernkop-Schnurch, Development and in vivo
evaluation of an oral insulin–PEG delivery system. Eur. J. Pharm. Sci., 22, 315–323, 2004.
89. D.Guggi, A.Bernkop-Schnurch, Systemic peptide delivery via the stomach: in vivo evaluation of an oral dosage form for salmon calcitonin. J. Control. Rel. 92, 125–135, 2003.
90. A.Bernkop-Schnu¨rch, D.Guggi, C.Huck, The use of thiolated polymers as carrier matrix in oral peptide delivery – proof of
concept. J. Control. Rel., 106, 26-33, 2005.
91. A.Bernkop-Schnurch, Mucoadhesive systems in oral drug Delivery, Dr Drug delivery/formulation and nanotechnology, 2,
83-87,l2005.
92. L. Illum., Nasal drug deliver-possibilities, problems and
solutions., J. Control. Rel., 87, 187-198, 2003.
93. H. Kublik, M.T. Vidgrenb., Nasal delivery systems and their effect on deposition and absorption., Adv. Drug Del. Rev., 29, 157–177,
1998.
94. S. Gizurarson, E. Bechgaard, Intranasal administration of insulin to humans, Diabetes Res. Clin. Pract. 12, 71-84, 1991.
95. P. Arora, S. Sharma, S. Garg, Permeability issues in nasal drug delivery, Drug Discov. Today, 7, 967–975, 2002.
96. H.L. Luessen, J.C.Verhoef, A.G. de Boer, H.E. Junginger, B.J.de Leeuw, G. Borchard, C.-M. Lehr, Multifunctional polymers for the peroral delivery of peptide drugs, in: E. Mathiowitz,D.E.
Chickering III, C.-M. Lehr (Eds.), Bioadhesive Drug Delivery Systems. Fundamentals, Novel Approaches, and Development,
Marcel Dekker, New York, 299– 339, 1999.
97. V. Dodane, M. Amin Khan, J.R. Merwin, Effect of chitosan on epithelial permeability and structure, Int. J. Pharm., 182, 21–32,
1999.
98. J.S. Park, Y.K. Oh, H. Yoon, J.M. Kim, C.K. Kim, In situ gelling and mucoadhesive polymer vehicles for controlled intranasal
delivery of plasmid DNA, J. Biomed. Mater. Res., 59, 144–151, 2002.
99. J. Wang, S. Sakai, Y. Deguchi, D. Bi, Y. Tabata, K. Morimoto, Aminated gelatin as a nasal absorption enhancer forpeptide drugs: evaluation of absorption enhancing effect andnasal mucosa
perturbation in rats, J. Pharm. Pharmacol. 54, 181– 188, 2002.
100. V. Leitner, D. Guggi, A. Bernkop-Schnurch, Thiomers in non-
invasive peptide delivery: in vitro and in vivo characterisation of a polycarbophil–cysteine/glutathione gel formulation for hGH,
J. Pharm. Sci. 93,1682– 1691, 2004.
101. W.H. Frey, Interview, Reuters Health, 16th February. M. Dahlin, U. Bergman, B. Jansson, E. Bjork, E. Brittebo Transfer of
dopamine in the olfactory pathway following nasal administration in mice, Pharm. Res., 17, 737–742, 2001.
102. S.C. Quay, Successful delivery of apomorphine to the brain following intranasal administration demonstrated in clinical study. PRNewswire. July 18th-2001.
103. S. Okuyama, The first attempt at radioisotopic evaluation of the integrity of the nose–brain barrier, Life Sci., 60, 1881–1884, 1997.
104. I. Derad, K. Willeke, R. Pietrowsky, J. Born, H.L. Fehm, Intranasal
angiotensin II directly influences central nervous regulation of blood pressure, Am. J. Hypertens. 11, 971–977, 1998.
105. L.Illum, Nasal drug delivery: new developments and stratagies., 7, 1184-1189, 2002.