definition of spectrum of sepsis pathophysiology of sepsis early goal directed therapy
TRANSCRIPT
SEPSIS AND EARLY GOAL DIRECTED
THERAPY
Goals of this didactic
Definition of spectrum of sepsis Pathophysiology of sepsis Early Goal Directed Therapy
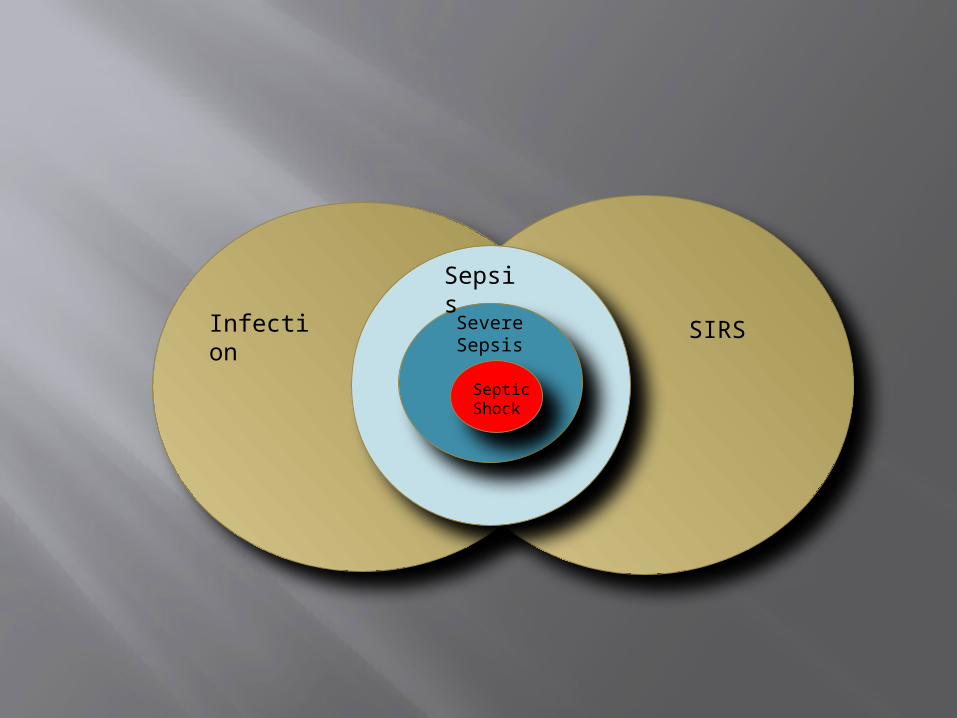
Infection SIRS
Sepsis
Severe Sepsis
Septic Shock
Basic Definitions
Infection: Pathophysiologic abnormality caused by a
microbial pathogen
Systemic Inflammatory Response Syndrome (SIRS) > 2 of the following:
Temp > 380C (100.4 F) or < 360C (96.8 F) Pulse > 90 RR > 20 (or PaCO2 < 32) WBC > 12,000 or < 4,000 or > 10% bands CRP or procalcitonin > 2 SD above normal
Basic Definitions
Sepsis: Presence of infection + SIRS
Documented OR presumed infection
Severe Sepsis: Sepsis + end organ dysfunction
End-Organ Dysfunction
Signs of Hypoperfusion Lactic acidosis or Mottling
Altered Mental Status Arterial Hypoxemia (PaO2:FiO2 < 300) Coagulation abnormalities (INR > 1.5) Thrombocytopenia (Platelets < 100,000) Ileus Renal, liver, cardiac failure
Lab or vital sign abnormalities
Septic Shock
Septic Shock: Sepsis + refractory hypotension
Hypotension: SBP < 90 MAP < 65 Decrease of 40 mm Hg SBP off baseline
Refractory Hypotension: Hypotension despite 20 - 40 mL/kg crystalloid
challenge
Pathophysiology of Sepsis
Lipopoloysaccharides and other bacterial components activate neutrophils and vascular endothelium
Cytokines and complement activation lead to vascular instability
Increase in tissue factor leads to microvascular occlusion
Combination leads to coagulopathy, vasodilation and capillary leak
Antimicrobial Therapies – ASAP!
Early antibiotic therapy (within 1 hour of presentation) decreases mortality
Check hospital antibiogram Target the most likely source Start broad, narrow later When all else fails:
Cefepime 1 gm IV and Vancomycin 15mg/kg Note: generally, anaerobes are NOT a cause of
sepsis except in rare intraabdominal cases
Early Goal-Directed Therapy
Algorithmic approach to management of severe sepsis Inclusion: 2/4 SIRS, SBP ≤90 after fluids or
serum lactate >4 Then randomly assigned to standard therapy or
EGDT
With their EGDT protocol: Reduction in sudden cardiovascular collapse
Mortality reduction: Standard therapy in-hospital mortality: 46.5% EGDT in-hospital mortality: 30.5%
16% Absolute reduction in mortality
Who’s eligible for EGDT?
Patients with severe sepsis with signs of hypoperfusion/end-organ dysfunction
Lactate > 4 mmol/L (The patient does NOT need to be
hypotensive)
Patients with septic shock
EGDT: Basic Principles
Goal-directed hemodynamic resuscitation of severe sepsis / septic shock:
Optimize CO: preload, afterload, and contractility
Restore systemic oxygen content Oxygen Delivery (DO2) = CO x CaO2 DO2 = CO x (1.34 * Hb * SaO2) + (0.003 * PaO2)
Preserve tissue perfusion
Avoid increases in myocardial O2 consumption
Specific Targets CVP of 8 – 12 mm Hg
Controversy about using CVP as no direct correlation to volume responsiveness
MAP of >65 mm Hg
UOP ≥ 0.5 ml/kg/h
Normalization of Lactate
ScvO2 ≥ 70% ScvO2 = from CVP SvO2 = from PA catheter
Optimize Preload
20-40ml/kg bolus
Looking for recruitable CO Increase in BP with fluid challenge
Pressors only after adequate fluid challenge
MAP Management
MAP <65
Fluid Challeng
ePressors
MAP Management
Vasopressors to MAP of > 65 Once initial fluid resuscitation
has been completed*
Arterial line placement is needed at some point
Pressors of choice Norepi +/- Vasopressin Epi
If patient does not respond to fluids and pressors, Hydrocortisone should be given
ScvO2 Management
ScvO2 <70
Transfuse to HCT
30
Inotropes
ScvO2 Management
Achieve ScvO2 ≥ 70% Initial fluid resuscitation Blood transfusions to HCT >
30%** 1 U PRBC will raise HCT ~ 3% or
Hgb 1 gram Inotropic therapy Decrease O2 consumption
Major users are muscles of respiration
Intubation, sedation, and paralysis may be needed
Inotropic therapy
Dobutamine Use when ScvO2 < 70% despite fluids and
HCT > 30% Improves contractility Use in combination with vasopressor because
of vasodilatory effect Dose: 2.5 to 20 mcg/kg/min Major adverse effect: dysrhythmias
Access
Central Access in order to follow ScvO2 Arterial Line: especially if patient requires
pressors Intubation if patient hypoxemic or with
significant altered mental status Early intubation can decrease oxygen
consumption by decreasing work of breathing
Time Frame
Within 3 hours: Get lactate level Blood cx Abx (within 1hour) Fluid resuscitation
Conclusion
Early recognition of sepsis is key in lowering mortality
Early antibiotics Early Goal Directed Therapy in
appropriate patients Appropriate access Being Aggressive